
Introduction
NHS performance across a broad range of measures remains worse than prior to the COVID-19 pandemic. The government has argued it has inherited a ‘broken NHS’ and that one of its key missions is to improve NHS performance.
One reason for poor NHS performance in recent years is the seemingly large fall in hospital productivity since the start of the pandemic. Put simply, the service is requiring more funding and more staff to deliver the same amount of hospital care. This year, for the first time, NHS England produced its own estimate of the productivity shortfall, estimating that acute hospital productivity in 2023–24 was 11% lower than pre-pandemic levels.
This is a problem not just for the health service and those wanting to use it, but also – due to the sheer size of the NHS – for the government’s fiscal position and for the broader economy. Accordingly, both the previous government and the new government have made improving NHS productivity a major focus. At the 2024 Autumn Budget, Rachel Reeves announced additional capital funding for the NHS and suggested that this would ‘enable the NHS to deliver 2% productivity growth next year’. Wes Streeting, the Health and Social Care Secretary, has reiterated this, saying the NHS has ‘got to improve productivity’ and that investment must be linked to reform.
In this comment, we examine what the latest data suggest about the state of NHS hospital productivity in England. We first show that hospital activity has increased substantially over the last year. We then show that this increase in activity is larger than the increase in hospital staffing over the same period. This suggests that hospital labour productivity, at least as measured by the number of patients treated per staff member, has increased over the last year. This improvement is welcome. It does, however, only partially offset previous reductions since 2019, leaving hospital productivity still substantially below pre-pandemic levels.
Throughout this comment, we focus on hospital productivity in England. This necessarily paints an incomplete picture – it excludes changes in primary care, for example, and excludes developments in Scotland, Wales and Northern Ireland. But it provides a valuable insight into what is happening inside a large and important sector of the NHS, for which we have detailed data.
What has happened to hospital activity over the last year?
Over the last year, there has been a considerable increase in the number of patients treated by NHS hospitals. Figure 1 shows how various measures of hospital activity have changed over time relative to their pre-pandemic levels. All measures of hospital activity show substantial growth so far this year (the purple bars are all above the dark grey bars) and all measures are now above their pre-pandemic levels (all purple bars are positive). For emergency admissions, 2024 is the first year to exceed pre-pandemic activity levels.
Figure 1. Change in NHS hospital activity since 2021 relative to 2019
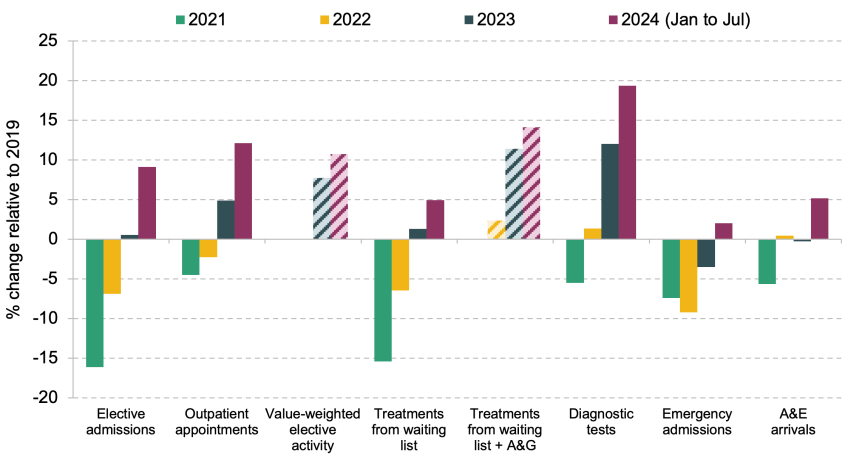
Note: Striped bars indicate that those activity measures have shorter time periods of data available. Value-weighted elective activity data are only available from April 2023 to March 2024 (measured relative to the same period in 2019–20). Treatments from waiting list + A&G (advice and guidance) diversions data are available from April 2022 to March 2024 (also measured relative to the same period in 2019–20). All other variables are reported as totals for the year (2021 to 2023) or for the seven months to July (2024) relative to the same months in 2019. A&E arrivals are for type 1 major A&E departments. Outpatient appointments are attended appointments.
Source: Authors’ calculations using NHS Digital’s monthly Hospital Episode Statistics for admitted patient care, outpatient and accident and emergency data (2024), NHS England’s referral to treatment (RTT) waiting times (2024), NHS England’s diagnostic waiting times and activity statistics (2024), NHS England’s recovery of elective activity management information (2024), and NHS England’s A&E attendances & emergency admissions statistics (July 2024).
Elective activity – pre-planned admissions and outpatient appointments – has increased by more than other types of hospital care. Elective activity is even further above pre-pandemic levels after adjusting for the cost of the different types of elective activity provided (value-weighted elective activity). This adjusts for the large difference in cost between an average elective admission and an average outpatient appointment, as well as changes in the types of appointments and admissions delivered, which can also differ in complexity and hence cost. This suggests that the NHS is not only treating more elective patients but is also providing more complex treatment on average, likely reflecting an increase in the average severity of patients (and, perhaps, some change in how patients are coded). Even this could understate the increase in NHS activity levels, as it fails to account for the growing amount of care provided outside of hospitals. This does not matter for hospital productivity, the focus of this piece, but does matter for an evaluation of broader NHS performance. For example, advice and guidance services provide specialist advice to GPs, ‘enabling a patient’s care to be managed in the most appropriate setting, strengthening shared decision making and avoiding unnecessary outpatient activity’. If we also account for advice and guidance services, elective activity is even further above pre-pandemic levels (labelled as ‘Treatments from waiting list + A&G’ in Figure 1). The NHS is also carrying out far more diagnostic tests than it was prior to COVID-19.
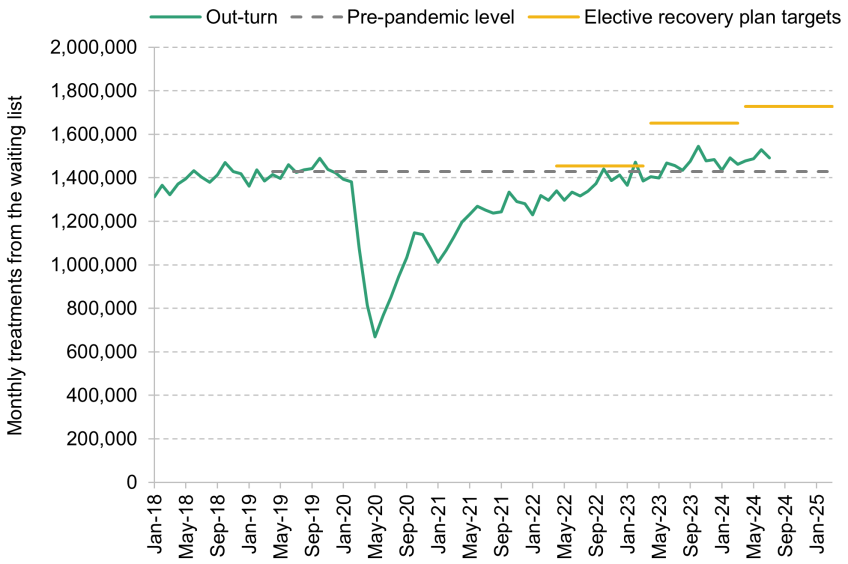
Of particular interest to policymakers, given the focus on achieving reductions in waiting times, is the number of treatments from the elective waiting list. Over the first seven months of 2024, the NHS treated around 5% more people from the waiting list than during the same period in 2019 (a more modest increase than seen for elective activity as a whole). To put this in context, in 2022, NHS England set out its elective recovery plan. One key target was to achieve a 20.9% increase in elective activity relative to 2019–20 by 2024–25 (with intermediate targets for earlier years). While treatments from the waiting list are no longer below their pre-pandemic levels, and are growing steadily, they still fall significantly short of the targets set out in the elective recovery plan, as shown in Figure 2.
Figure 2. NHS treatments from the elective waiting list (three-month rolling average)
Source: Authors’ calculations using NHS England, Referral to treatment (RTT) waiting times (2024) and National Audit Office, Managing NHS backlogs and waiting times in England (2022).
Where does this leave NHS hospital productivity?
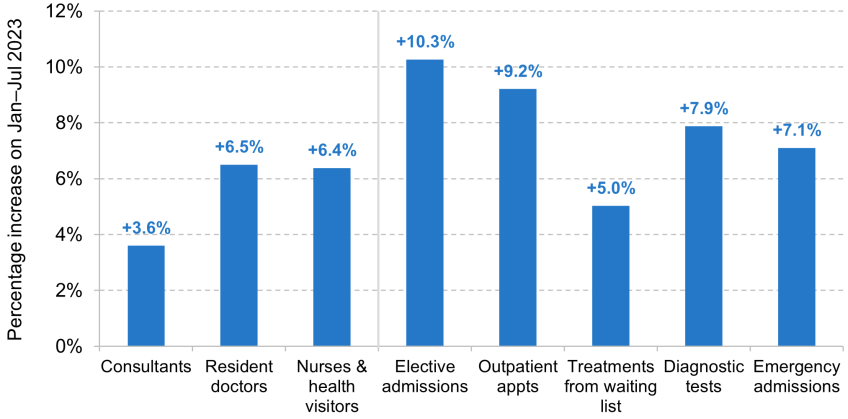
Higher levels of NHS activity are good news for a government hoping to reduce the waiting list, and good news for patients hoping to access care, but do not necessarily point to higher productivity: higher activity could just be the result of additional inputs (e.g. more staff). To explore this further, Figure 3 shows changes in NHS hospital and community staffing alongside changes in key measures of hospital activity. Panel a shows staffing and activity for all of 2023 (green bars) and for January to July 2024 (yellow bars) relative to the same months in 2019. To look just at more recent trends, Panel b shows the change in staffing and activity between January to July 2023 and January to July 2024.
Panel a shows that since the start of the pandemic, the number of clinical staff in the NHS (on the left-hand side) has increased by substantially more than all forms of hospital activity (on the right). This is true in both 2023 and 2024. For example, between January and July 2024, the NHS had 18.2% more consultants and 22.9% more nurses and health visitors than during the same period in 2019, but only delivered 9.1% more elective admissions and 12.1% more outpatient appointments. As we have previously argued, this suggests that hospital labour productivity (i.e. treatments per staff member) is substantially lower than pre-pandemic, consistent with the findings of NHS England in its own analysis. The same is true if we use a measure of value-weighted elective activity (not shown on the chart), suggesting that this fall in measured labour productivity cannot all be explained by changes in the complexity of treatment delivered.
Figure3. Change in NHS hospital and community staffing and hospital activity
Change between January–December 2019 and January–December 2023, and between January–July 2019 and January–July 2024

Change between January–July 2023 and January–July 2024
Source: Authors’ calculations using NHS Digital’s NHS workforce statistics (2024), in addition to sources from Figure 1.
Turning to Panel b, both hospital staffing and activity have been higher over January to July 2024 than in the same months last year. However, activity has – in most cases – increased by more than staffing. For example, while the number of full-time-equivalent consultants has risen by 3.6% and the number of nurses and health visitors has risen by 6.4%, the number of elective admissions has risen by 10.3% and the number of outpatient appointments has risen by 9.2%. This has not translated in full to additional treatments from the waiting list (‘clock stops’, which are 5.0% higher than a year earlier). Nonetheless, taken together, these figures suggest that hospital labour productivity is higher in January to July 2024 than over the equivalent period in 2023. However, as Panel a shows, hospital labour productivity in 2024 remains substantially lower than in 2019 (as activity over those five years has grown by less than staffing).
What has caused this welcome part-reversal? A full analysis is beyond the scope of this comment (and indeed very challenging to do in general), but we can nonetheless rule out two of the more obvious potential explanations.
First, one commonly cited explanation for reductions in NHS productivity (including, it should be said, by some of the authors of this comment) has been a change in the NHS ‘input mix’: the fact that clinical staff numbers have increased dramatically, but without a commensurate increase in other inputs, such as hospital beds, equipment and manager numbers. But over the past year, the number of hospital beds has grown more slowly than the number of clinical staff, and the number of managers has grown at a similar rate. The maintenance backlog has continued to grow, and capital funding has been siphoned off to meet day-to-day spending pressures. Therefore, it does not seem that the NHS ‘input mix’ has decisively shifted back towards non-frontline-staffing inputs, and so this would not appear to explain all of the recent improvement in productivity.
Second, industrial action is often used as an explanation for the productivity challenge: NHS England estimates suggest that it contributed substantially to poor productivity performance in 2023–24, for instance. But strikes continued throughout the first half of 2024, with the junior doctor pay dispute not resolved until the end of our analysis period, in July 2024. The end of industrial action therefore cannot explain the recent improvement in our simple measure of productivity (though should lead to productivity improvements later in the year).
The explanation instead would appear to lie elsewhere. A greater focus on the issue from policymakers – including then-Chancellor Jeremy Hunt in the Spring 2024 Budget, and senior NHS England leadership – and from hospital managers might have spurred efforts to use staff more efficiently. The Elective Recovery Fund and the move to payment by results (PbR) for elective activity, where NHS providers are paid per unit of activity they have delivered, may have strengthened the incentives for providers to deliver elective care, and potentially to increase their productivity. Some of the increase in measured activity – particularly value-weighted activity – could be due to changes in the way data are recorded and coded. There may be some natural reversion to the pre-pandemic level of productivity as the impacts of the COVID-19 pandemic continue to fade away. Ultimately, more work is needed to understand these trends.
Conclusion
Over the last year, there has been a substantial increase in the number of patients treated by NHS hospitals in England. This increase in activity is greater than the increase in clinical staffing over the same period, which suggests that there has been an improvement in the productivity of staff within those hospitals. This has not translated into quite as many treatments from the waiting list as we might have expected, and the NHS is still lagging behind its elective recovery plan, but it is at least heading in the right direction.
While this is unequivocally good news, and while the new government will no doubt welcome the propitious timing of this improvement, we should see it in context. NHS hospital productivity remains substantially below pre-pandemic levels. The productivity increase between last year and this year will not on its own deliver the scale of improvements in NHS performance promised at the election. NHS targets for increasing the number of treatments from the waiting list, produced as part of the previous government’s 2022 elective recovery plan, are still very likely to be missed this year. And at the current rate, you would need several more years’ improvements just to return the NHS to its pre-pandemic productivity levels, let alone exceed them. The NHS workforce plan is built on the assumption that the NHS can deliver continual improvements in labour productivity – without these, even the large planned increase in the NHS workforce would not, according to the service’s own estimates, be enough to meet demand for care.
Nonetheless, there are reasons for optimism. An increase in hospital productivity between last year and this year shows that future increases are possible, and perhaps starts to assuage worries about long-term scarring from the COVID-19 pandemic. A rise in productivity in 2024 would certainly be a much better base from which to build than a situation where productivity had again fallen. We have long argued that a shortage of capital investment could in part explain recent productivity challenges; at the Autumn Budget, Rachel Reeves prioritised NHS capital investment, a welcome move that ought to deliver future benefits. Industrial action has also come to an end, which will provide a one-off productivity boost. There is therefore good reason to expect continued NHS productivity improvements in the coming years, though there is absolutely no room for complacency.
Authors

Olly Harvey-Rich
Olly joined the IFS in 2024 and works in the Healthcare sector.

Max Warner
Max joined the IFS in 2020. His work covers health and social care, public spending and public sector productivity.

More from IFS
Understand this issue



Policy analysis



Academic research


