
Downloads
Download the report as a PDF
PDF | 572.62 KB
Executive summary
More than 1.5 million staff work for the NHS in England, across a wide range of occupations. Progression within these occupations – for example, from nurse to senior staff nurse – has long been a focus of workforce policy in the NHS. Transitions between broad occupation groups – such as healthcare assistants who train to become nurses – are less prominent, but have become increasingly common over time. For staff members, these transitions can provide important opportunities for career progression and development, whilst for NHS trusts they can be a valuable way to fill ‘skills gaps’ with staff they already know well. They might also be a way for the NHS to invest more in the skills and workforce of its local communities, an ambition emphasised in the recent ‘10 Year Health Plan for England’. However, there is little large-scale evidence to date on these types of transitions in the NHS, making it difficult to judge how far they can contribute to each of these goals.
In this report, we use data from the Electronic Staff Record (ESR), the monthly payroll of the NHS, to set out which staff transition between which occupations, and how this has changed over time. We place a particular focus on transitions from clinical support occupations – such as healthcare assistants and nursing auxiliaries – to registered clinical occupations, such as nurses, midwives and physiotherapists. Recent governments have created new routes into nursing that have a particular policy focus on recruiting from clinical support roles into registered nursing roles, and these transitions are now a much bigger source of nurse recruitment. However, they remain much more common in some NHS trust types and some parts of the country. We analyse how the local labour market might affect the frequency of these transitions and discuss the implications for future workforce policy.
Key findings
- Career pathways in the NHS are typically within a single occupation, especially for those who have spent a long time in training, such as doctors and nurses. However, for clinical support staff, training in a new profession within the NHS has become an increasingly common way to access professional qualifications, greater autonomy and higher pay. Of the cohort of clinical support staff working in the NHS in 2010, 8% were working in the NHS in a different occupation group four years later; for the 2020 cohort, this share had doubled to 16%.
- The share of clinical support staff moving into registered nursing within four years has tripled in the last decade, from 2% in 2010 to 6% in 2020. Nursing is now the most common destination occupation for clinical support workers who change occupation within the NHS. Promoting these transitions has been a key policy objective of introducing nursing degree apprenticeships and the nursing associate role.
- Increasing rates of transitions to nursing have meant that 16% of the new nursing cohort in 2024 were recruited from a clinical support role in the NHS, up from 4% in 2014. In contrast, the share of registered allied health professionals – such as physiotherapists, radiographers and occupational therapists – recruited from among clinical support staff has remained relatively stable at around 10%.
- Early cohorts of registered staff recruited through an occupational transition within the NHS have had higher retention rates than staff recruited externally. 54% of the 2014 cohort of registered staff recruited from outside the NHS were still working in NHS hospitals and community care in 2024, compared with 63% for those recruited from another NHS role. In contrast, initial evidence on the retention of recent cohorts shows almost no differences – although it is too soon to judge whether this is a decisive break in the previous pattern.
- Many common starting points for occupational transitions, such as degree apprenticeships or the nursing associate role, have seen large increases in the numbers of new starters in the last few years. Over 1,000 staff started a nursing degree apprenticeship in 2024, compared with just over 300 in 2019. Since these staff are still largely in training, we can expect rates of transitions to registered roles to continue to rise – as long as there are jobs for them to move into.
- One policy objective of encouraging occupational transitions emphasised in the recent NHS 10-Year Plan is that they can widen access to higher-paying careers in disadvantaged areas of the country. However, we show that transitions are much more common in areas where wages are higher in the wider (non-NHS) labour market. In 2023, clinical support workers in the South East were nearly twice as likely to move into a registered profession as those in the North East. Trusts in higher-wage areas often see higher vacancies and more competition for staff. This may make these trusts more willing to bear the costs of supporting and funding these opportunities.
- Of the ten trusts with the highest rates of occupational mobility since 2019, nine are mental health & learning disability trusts. These trusts require more specialised skills and tend to see higher vacancy rates. Offering pathways into specialised registered clinical occupations, such as mental health nursing, may therefore act as an important mechanism to attract and retain staff.
- The government’s 10-Year Plan sets out an ambition to further expand routes into registered occupations. Whether trusts will be willing to do so will depend on how easily trusts can recruit and retain staff through other routes. If the government wants to incentivise trusts to offer and promote occupational retraining, it will likely face trade-offs between targeting trusts with the most pressing workforce gaps and achieving broader objectives such as reducing regional inequalities in training opportunities and social mobility.
1. Introduction
Many careers in the NHS are spent within a single occupation group, supported by well-established institutional structures around training, pay and progression. These structures, often shaped by professional bodies such as the Royal Colleges, provide clear pathways for development within occupations. A nurse, for example, may begin as a student, qualify and progress to senior clinical or managerial roles within nursing.
In this report, we focus on staff changing occupation within the NHS, and particularly moving from support roles into registered clinical professions. This has been an area of increased policy focus for governments of all stripes over the past decade. The previous government introduced new training routes, such as the nursing degree apprenticeship, and new roles, such as nursing associates, that provided a bridge between healthcare assistant roles and registered nursing (Warner et al., 2023). A commitment to expanding routes into clinical professions was renewed in last summer’s ‘10 Year Health Plan for England’.
There are a number of reasons trusts might want to make it easier for staff to move between occupation groups. One reason to expand these routes is to broaden access to registered clinical professions. The 10-Year Plan set out an ambition to ‘transform the NHS into a force for social mobility and local prosperity’, including by expanding the offer of nursing apprenticeships (Department of Health and Social Care, 2025). If these routes can enable staff to access qualifications and careers they otherwise would not have, these policies could act to improve social mobility.
Another stated aim of promoting occupational transitions is to improve retention or, more generally, to make the NHS a more attractive employer. Opportunities for training, career progression and pay growth could make staying in an existing role more attractive; or staff might be less likely to leave having switched to an occupation group that suits them better. NHS Employers (2024a) discusses improvements in retention as a key benefit to rolling out apprenticeships.
Whilst each of these aims might be a good reason to promote occupational transitions, making these transitions easier will not automatically achieve all of them. In each case, the effects depend crucially on the incentives of trusts to offer opportunities, which staff are offered and take up these transitions, and under what conditions. If staff who move occupation group are not those with otherwise worse access to career progression, these routes may have little impact on social mobility. Similarly, the staff who take up these opportunities could be those who would otherwise have had high levels of retention.
This report investigates which staff are most likely to move between occupation groups in the NHS, and some of the consequences both for their own careers and for their employers. We examine first which types of staff tend to see higher rates of transitions between occupations, and how this varies over time and at different types of trust. We then analyse why similar staff in different parts of the country seem to move occupations at strikingly different rates, and discuss the potential consequences of these differences, including for retention and recruitment in the staff groups they join. Finally, we consider what these patterns suggest for policymakers should they wish to increase these pathways further.
Our main data source for the analysis in this report is the Electronic Staff Record (ESR), the monthly payroll for all staff directly employed by the NHS. This includes all NHS trusts but does not include staff employed in primary care. These data allow us to track the careers of most NHS staff over the period between 2010 and 2024, and include detailed information on pay, hours worked, demographic characteristics and job characteristics.
The rest of the report is organised as follows. In Section 2, we describe our data in more detail and set out our definitions of occupational transitions. In Section 3, we document the staff groups that see the most frequent transitions and we examine trust-level variation in transition rates. In Section 4, we analyse the relationship between the outside labour market and the frequency of occupational transitions. In Section 5, we discuss the consequences of these transitions for recruitment and retention. Section 6 concludes.
2. Data and definitions
The Electronic Staff Record
The main data source for our analysis is the Electronic Staff Record (ESR), which is the monthly payroll system covering all staff directly employed by the NHS. It includes all staff directly contracted to NHS organisations but excludes those working in primary care, such as staff working for a GP practice, and those employed by outsourced providers, such as porters or cleaners in some hospitals.
We use data for the period between January 2010 and December 2024, allowing us to follow individual staff members across their employment in the NHS over a period of 15 years. In all cases, the data are pseudonymised: names and identifying information (such as addresses or National Insurance numbers) are removed, and individuals are tracked over time using unique, non-identifying codes.
Each monthly ESR record contains detailed information on staff characteristics, job roles, hours and earnings. It reports both contracted and worked hours, grade and pay band, and provides a breakdown of basic pay and additional payments (e.g. from bank work, high-cost area allowances or performance-related pay). The data also include demographic and job characteristics such as age, gender, self-reported ethnicity, employing trust, start date, job role and any recorded absences. Importantly for this analysis, job roles are recorded at a high level of detail and according to a nationally consistent coding scheme.
Defining occupational transitions
Many staff move between positions in the NHS with different formal job titles in a way that is not well described as an ‘occupational transition’. For example, a registered nurse might progress to becoming a matron or nurse consultant. In this report, we are interested in transitions between different types of occupation, such as those that involve a different set of qualifications or training.
We therefore group job roles into seven broad categories, using both NHS Staff Groups and prerequisite qualifications to define groups. Our main analysis will consider movement from one of these groups to another as an ‘occupational transition’. These groups are as follows:1
- registered ambulance staff (such as paramedics);
- administration and estates staff;
- registered nurses and health visitors (including nurse learners);
- registered midwives;
- qualified allied health professionals (AHPs, such as radiography, physiotherapy and occupational therapy; including students and trainees);
- qualified Healthcare Science and Public Health scientific staff (including students and trainees);
- clinical support staff (including healthcare assistants, support workers, nursing assistants, and any other non-registered support staff in patient-facing roles).
We omit doctors from our analysis as they are, unsurprisingly, very unlikely to switch occupation within the NHS.
Some types of occupational transition will take place within these groups and will not be captured by our analysis. For example, a qualified physiotherapist who retrains in a different allied health profession will appear to stay within one group. However, moves between these groups almost certainly reflect a significant change in occupation and are very unlikely to be an automatic feature of a training pathway. For this reason, we include students and trainees in the job groups in which they are training.
Five of these groups (all except clinical support staff and administrative/estates staff) are defined in terms of professional registration or qualification. Transitions to ‘registered professions’ refer to these five groups. These transitions – a form of progression that increases pay, autonomy and qualifications – are of particular interest economically and for policymakers, and we will say much more about them, their drivers and their consequences in the following sections.
We make two further restrictions to our definition of occupational transitions. First, we exclude observed moves from one group to another where the first role had been held for less than a year. This type of move is common among, for example, internationally recruited nurses who formally hold a non-registered position for a short period whilst their registration is processed. This represents an administrative change only, as these staff members were essentially recruited to be nurses. Second, we exclude ‘return transitions’, where the destination job role had been held within the last three years. Together, these restrictions generate a sample of 319,000 transition events over our 15-year study period, around two-thirds of the ‘raw’ observed transitions.
3. How common is occupational mobility?
We first consider how frequent occupational transitions within the NHS are for different groups of staff. Not all staff members are likely to face the same set of opportunities to change role, and take-up of these opportunities might differ across staff groups. We therefore examine differences in transition rates across occupation groups, demographic characteristics and trust types.
Which staff are most likely to change occupation?
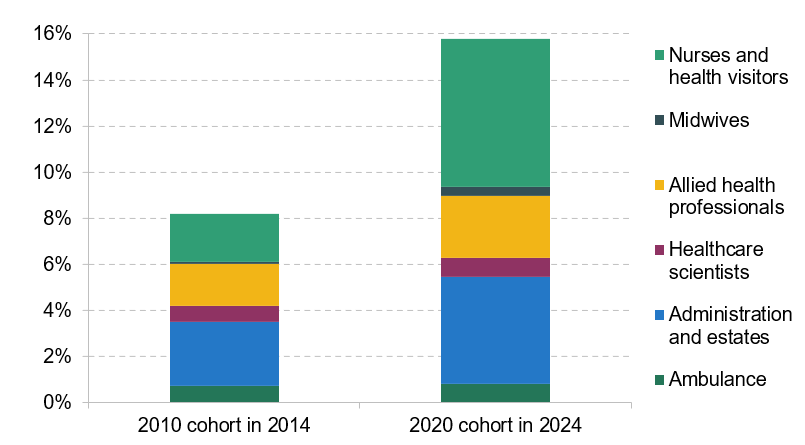
NHS staff in some occupation groups are much more likely than others to transition to another group. Figure 1 shows how likely a staff member in a given occupation group is to have transitioned to a different group four years later. The left panel looks at a cohort of staff in 2010 – the earliest we observe – and tracks their transitions by 2014. The right panel does the same for the latest cohort in our analysis (from 2020 to 2024).
Figure 1. Staff transitions after four years, by occupation group

Note: ‘Left hospital and community sector’ includes both transitions to primary care and NHS exits.
For all staff, switching occupation group is less common than either staying in the same group or leaving the NHS hospital and community sector altogether. Given the time and effort involved with making an occupational transition, especially in the earlier period, this is not particularly surprising. Exits here may involve an occupational transition to a non-healthcare role, but many will not. The most common destination for nurses, for example, is to remain in a nursing role in the private or voluntary sectors (Shembavnekar and Kelly, 2023). Exits to non-healthcare roles are more common for support staff (Kelly et al., 2022).
However, Figure 1 also shows that occupational transitions have become significantly more common over time for clinical support workers, and are more common for this group than for any other. The share of clinical support staff who transitioned to another occupation group within four years rose from 8% in the 2010 cohort to 16% in the 2020 cohort. This partly reflects a deliberate policy effort and the introduction of new pathways, such as nursing degree apprenticeships and nursing associate roles in 2017. Survey evidence also suggests a high underlying demand for routes into registered professions for clinical support staff (Kessler et al., 2021).
Nurses and health visitors – a group that have already invested into a long training pathway – are the least likely to transition to a different occupation. For all groups other than clinical support workers in Figure 1, transition rates have remained roughly constant across cohorts. Midwives, for example, were roughly as likely as clinical support staff to switch occupation group in 2010, but have subsequently seen a much smaller increase in transition rates. This pattern suggests that deliberate policy efforts to create routes from support roles into registered occupations have played a significant role in shaping the frequency of occupational transitions in this period.
Occupational transitions as progression
When comparing occupational transitions within the NHS with those in the wider labour market, within-NHS transitions stand out for rarely involving a downward move in terms of earnings and seniority, as captured by the Agenda for Change (AfC) pay scale. Across occupational groups, fewer than 1 in 10 occupational transitions involve a move to a lower AfC band. We note that progression up the AfC scale does not just imply higher earnings – itself an important outcome – but also additional skills, responsibilities and autonomy.2
This contrasts with findings in the wider economy (Longhi and Taylor, 2013; Forsythe, 2023), where workers transitioning to a new occupation – often in response to job loss – commonly have to ‘start over’ on lower pay, complexity and seniority.
For clinical support staff in particular – a group that is essentially ‘capped’ at AfC Band 4 – occupational transitions to registered roles in nursing or one of the allied health professions are a key route to further progression in terms of gaining qualifications, taking on more responsibilities and earning more.3 Figure 2 shows the range of destinations for the 2010 and 2020 cohorts of clinical support workers. Nursing and allied health professions are an important destination for both cohorts, with transitions to nursing having grown substantially during this period. This increase coincides with both the expansion of new routes into nursing (such as degree apprenticeships), and the previous government’s target to recruit 50,000 new nurses (Department of Health and Social Care, 2020).
Figure 2. Occupation groups of clinical support staff who switch occupation after four years
Note: ‘Cohorts’ defined, as in Figure 1, to mean all staff employed in a clinical support role in 2010 or 2020, respectively .
These transitions from clinical support roles to registered roles are therefore not just one of the most common types of occupational transition, but also one of the most economically interesting as a route to additional training and increasing autonomy at work, as well as earnings growth. Their expansion has been a key focus of explicit policy efforts in the last 15 years, and they will be central to ambitions for the NHS to be a ‘force for social mobility’ going forward. In the rest of this report, we therefore concentrate on these types of transitions. More specifically, we consider which clinical support staff have been most likely to move into registered professions, the possible drivers of these differences, and what the impacts have been for these staff and their employers.
Who transitions?
There are a number of differences in transition rates between different demographic groups. Men and women see similar rates of transition from clinical support roles to registered roles overall, but their destinations are often different. Women are more likely to transition to nursing roles than men: we see around 9 transitions per 1,000 women in clinical support roles to nursing roles per year, compared with 6 for men. In contrast, we see many more transitions to registered ambulance roles for men (5 per 1,000, compared with 1 per 1,000 for women); and similar numbers of transitions to allied health professions for workers of either gender (around 7 per 1,000).
Transitions are most common among support workers in their mid 20s, and decline steadily with age thereafter. The rate of transitions to nursing is more than five times higher for 25-year-old support workers than for 50-year-old ones, with a narrower gap for transitions to allied health roles.
There are some differences by ethnicity: clinical support staff from Black African backgrounds are more likely to transition to a registered clinical role than those from other large ethnic groups. While staff members from White and Indian backgrounds are similarly likely to make a transition overall, the destinations differ: clinical support staff from Indian backgrounds are more likely to transition to nursing, whereas White staff are more likely to transition to the allied health professions. This matches the overall ethnic composition of nurses relative to allied health professions (NHS Digital, 2023).
In this report, we focus on differences in the frequency of transitions across trusts in different parts of the country, rather than across individuals. However, it will be important to account for differences in the composition of clinical support staff across regions. In Section 4, we will therefore go on to ask whether staff with similar characteristics are more likely to transition to a registered clinical profession in some parts of the country, and why this might be the case.
How much do rates of transition to clinical professions vary across trusts?
Around three-quarters of transitions from clinical support roles to registered clinical roles happen within the same NHS trust. It is less common for staff members to switch to a new trust for their first registered role. In some trusts, many more clinical support workers progress to registered roles than in others. Figure 3 illustrates the wide range of transition rates. At the bottom end, some trusts saw an average of 0.5% of clinical support staff move to qualified clinical roles each year, while at the top end, 6% moved.
Figure 3. Rates of occupational mobility from clinical support staff by trust, 2019–24

Note: Excludes two trusts with fewer than 10 observed occupational transitions in each year.
Although high transition rates are found across all types of trusts, mental health and ambulance trusts are clustered near the top of the distribution. Nine of the top ten trusts, on this measure of occupational mobility, are mental health & learning disability trusts. These differences will reflect variation in which trusts offer support and funding for occupational transitions, as well as differences in the demand for them from staff.
On the supply side, there is evidence that mental health trusts find it harder to recruit, with persistently higher vacancy rates than other areas of the NHS (Gilburt and Mallorie, 2024). Offering routes into registered professions is one available mechanism that could boost recruitment and retention in these hard-to-fill roles. The clinical associate in psychology role, which involves a degree apprenticeship, was introduced in 2020 as one way to address this type of need (O’Driscoll et al., 2024). Some case studies from trusts similarly suggest that offering these routes to registered professions has been ‘a major benefit to recruitment’ (NHS Employers, 2024b). On the demand side, staff working in specialised areas such as mental health or ambulance care may be particularly motivated to pursue further qualifications.
In line with the national trend, almost all trusts have seen growing rates of occupational mobility over time. A ranking of trusts along this measure is not completely static but, on average, trusts with high transition rates in the early part of our study period tend to still have high rates in the later years. Half the trusts in the top 25% for occupational mobility in 2011 were still in the top 25% ten years later, and only 12% had moved to the bottom 25%.
Trusts that were early adopters of the nursing associate role also tend to have high rates of transitions from clinical support staff to registered roles in general. This pattern persists several years later, after the roll-out of nursing associates had been completed nationally: a very small number of trusts that hired their first nursing associates in 2017 had an average transition rate of 17 per 1,000 in 2023, compared with 15 per 1,000 for 2018 adopters (which account for the bulk of trusts) and 10 per 1,000 for 2019 adopters (who hired their first nursing associates relatively late).
These persistent differences across trusts naturally lead to the question of what type of trusts, in what parts of the country, have these higher rates of clinical support staff progressing into registered clinical roles. In the next section, we focus on differences across trusts in different parts of the country, and explore how they relate to differences in local labour markets.
4. Is occupational mobility affected by the local labour market?
The NHS 10-Year Plan, published last summer, included an ambition to make the NHS into a ‘force for social mobility and local prosperity’. Providing routes to move into clinical professions from clinical support roles – which have lower pay and require fewer formal qualifications – is one mechanism that might aid social mobility via the NHS. In this section, we describe how the use of this mechanism has been distributed across the country thus far, and examine the role of job opportunities outside the NHS.
Geographic patterns in the frequency of occupational transitions will be driven both by the rate at which trusts offer, promote and fund these pathways (the ‘supply side’) and by how interested staff are in taking them up (the ‘demand side’). In Section 3, we saw that occupational transitions were much more common at younger ages and for some occupation groups, suggesting that these are important factors on the demand side. Other relevant factors are likely to include motivation and skills, which are harder to measure directly.
On the supply side, trusts are likely to promote these pathways when they are a cost-effective way to address their workforce needs, such as improving recruitment or retention. Offering these opportunities can be costly for trusts. Degree apprenticeships, for example, can involve trusts facing significant costs to pay for additional staff during teaching time (backfill), which usually cannot be funded using the apprenticeship levy (University Alliance, 2025). Trusts that find it easier to recruit staff through other routes, such as international recruitment or due to lower levels of competition from other employers, may find that funding these routes is not a cost-effective way to fill vacancies. This would be consistent with the finding in Section 3 that the highest rates of transition are in mental health trusts, which face some of the greatest challenges in filling vacancies.
If this hypothesis is true, we would expect to see opportunities for occupational transitions within the NHS concentrated in areas where jobs in the wider labour market are also well paid and offer good progression. This pattern would run counter to the policy objective of providing routes to formal qualifications and progression in areas with lower levels of such opportunities. On the other hand, the NHS – as a national organisation funded by general taxation, with relatively fixed pay scales across areas, and therefore perhaps less dependent on local economic conditions than other employers – may be able to offer more opportunities for occupational mobility specifically in areas where such opportunities are otherwise scarce. This would be especially valuable for policymakers keen to improve economic opportunities in disadvantaged areas.
In order to test these competing ideas, we analyse how rates of transition from clinical support roles to other clinical professions vary across areas, and how this relates to measures of pay and progression in the local area. To begin with, Figure 4 shows the rate of transition to registered clinical roles per 1,000 clinical support staff by local area of the trust. We define local areas in terms of Travel to Work Areas (TTWAs), a geographical unit that is designed to approximate local labour markets. This indicates that transitions are typically highest in London, the South and parts of the Midlands. Taken as a whole, the rate of transitions in the South East of England was nearly twice that in the North East in this period.
Figure 4. Rate of transition to registered clinical roles per 1,000 clinical support staff, 2023

Note: Areas shown in grey do not contain an NHS trust in our sample.
Some of this geographical variation will be explained by differences in the demand-side characteristics discussed above. For example, since the workforce in some areas (including London) is younger on average, we would expect to see more transitions in London than elsewhere, even if similar opportunities were available everywhere.
In order to examine differences on the supply side, we use regression methods in this section to assess how the frequency of transitions relates to local labour markets. In this way, we compare similar staff members in different regions, accounting for demographic characteristics including gender, age and ethnicity, so that comparisons between areas do not reflect any geographical differences in these characteristics. There will almost certainly be other demand-side differences between staff in different areas that we cannot observe, such as differences in people’s values, skills and goals. Therefore, our results should not be interpreted as ‘pure’ place effects. Nevertheless, they provide a guide to the types of places that tend to see higher rates of occupational mobility for staff members who are otherwise similar.
Are transitions more common when workers have better opportunities outside the NHS?
One possible reason for the differences in rates of transition seen in Figure 4 is that clinical support workers in some parts of the country have better alternative career options available to them. Training, and progression opportunities, including occupational transitions, are part of the ‘NHS offer’ to staff – which has to be competitive compared with that of other potential employers. Since NHS employers have relatively little scope to adjust pay within staff groups due to nationally set pay scales, improved progression and training options are a plausible way in which they might respond to stronger competition from other employers. There is evidence that this can lead to NHS employers offering faster progression within occupations in areas where competition for staff is stronger (Stoye and Warner, 2024).
Under this hypothesis, we would expect to see higher rates of transition in areas with higher-paying or otherwise more attractive alternative job opportunities for healthcare support workers. We would also expect to see more transitions in areas where there are many employers competing with each other than in areas where a small number of large employers can set the terms without much competition.
We test this hypothesis by estimating the relationship between measures of the outside labour market and transition rates to other clinical occupation groups among non-registered clinical support staff. In particular, we consider local measures of:
- pay for all workers in the low-paid labour market;
- pay for women in the low-paid labour market (since 77% of clinical support staff are female);
- wage growth over the last year for the average low-paid worker;
- wage growth over the last four years for the average low-paid worker;
- concentration of employers.
Details of how we define and construct these measures are provided in the technical appendix. In each case, we exclude NHS jobs from our measurements, to ensure that we are focusing only on the opportunities available outside of healthcare support workers’ current roles. Additionally, we focus on jobs around the 25th percentile of the non-NHS wage distribution, as an approximation of the segment of the labour market that competes with the NHS for these staff. Clinical support roles are paid between Band 2 and Band 4 of the Agenda for Change pay scale, which tends to fall between the 20th and 30th percentiles of the wage distribution in this period. This restriction allows us to approximate a set of relevant opportunities, rather than roles at the top end of the local pay distribution which may not be immediately accessible. We consider each of the listed variables in turn in separate regression models of transition rates, after stripping out the demographic variables discussed above and a ‘time trend’ capturing the rising rate of transitions nationally. This allows us to focus on area-specific associations for staff with similar characteristics.
Table 1 shows the results of these regression models. The coefficients should be interpreted as the additional number of transitions to registered roles per 1,000 non-registered clinical staff associated with a one-unit increase in the labour market variable. For example, staff working in areas with £1 higher hourly wages in the lower-paid labour market tend to see approximately 6 more transitions per 1,000, holding constant demographic differences. These effect sizes are meaningful relative to the overall transition rate: the average rate of transitions per 1,000 over the period we consider is 24.8.
Table 1. Local job opportunities and clinical support workers’ transitions to registered professions within the NHS

Note: Coefficients from a separate linear regression for each variable, also including age, age squared, gender, ethnicity, and time fixed effects. Wage growth variables are lagged by one or four years, respectively. Standard errors clustered at the Travel to Work Area level are displayed in parentheses.
*** p < 0.01; ** p < 0.05; * p < 0.1.
For more information on these measures and how they differ by area and over time, see our interactive data item Wages, pay growth and employer concentration in the labour market for lower-paid NHS staff.
The results suggest that transitions are significantly more common in areas with higher wages at the lower-paid end of the labour market. This evidence is consistent with the hypothesis that routes to occupational mobility are offered more frequently when competition for staff is stronger, even after adjusting for differences based on demographic composition and national trends over time.
There is no clear relationship with wage growth or employer concentration; if anything, the effects are slightly negative. One potential explanation of this finding is that in some parts of the country, wage growth at this part of the wage distribution is strongly linked to movements in the National Living Wage, which has risen quickly over the period we study. Since the National Living Wage plays a more important role in areas where wages overall are lower, this could mean that low-wage areas have seen especially fast wage progression – but this was driven by the rise in the National Living Wage, rather than by these areas being especially economically dynamic. In this way, the estimate could be conflating the effects of lower wages and higher observed wage growth.
In sum, it is staff in higher-wage areas who are more likely to transition to registered clinical professions within the NHS. To the extent that these transitions reflect routes to opportunity and social mobility for lower-paid staff, this suggests that wider regional inequalities are reproduced within the NHS. However, areas with higher wages are different from those with lower wages in many ways. Next, we dig further into the potential reasons for this pattern.
Why do higher-wage areas see higher rates of transitions?
Our findings show that the kind of areas with higher-paid alternative job opportunities also tend to see more occupational transitions within the NHS. This does not necessarily imply that the former is driving the latter, as this could be driven by local area characteristics that drive both NHS and non-NHS job opportunities. To better understand the mechanisms driving this relationship between outside wages and occupational mobility, we consider and test two plausible explanations:
- that trusts directly respond to changes in their local labour market with changes to their employment offer;
- that there are higher rates of registered staff recruitment more generally in higher-wage labour markets. This would mean that there are more occupational transitions into registered roles because there is a greater demand for staff, rather than occupational transitions making up a greater share of total employment in registered roles.
To test the first hypothesis, we strip out persistent differences in transition rates between areas from the associations estimated above. In other words, we remove any features of areas that do not change over our 12-year study period and may affect transition rates, such as the presence of an important local employer. The adjusted coefficients then reflect the association of changes in the regional labour marketwith changes in the frequency of occupational transitions in the NHS, all within the same area. If trusts respond to an increase in wages in their local area, for example, by offering more routes to registered professions, we would expect to see these effects here.
Figure 5 displays these results. There is no significant relationship between changes to any of the regional labour market characteristics and changes to transition rates into qualified clinical roles once permanent differences between areas are stripped out. This suggests that trusts and workers do not respond, at least in the (relatively) short term, to changes in these variables by changing the rates at which they offer or accept transition routes. Given the relatively long-term nature of the decision to invest in expanding these pathways, it is possibly unsurprising that year-to-year variations in outside wages do not seem to have much effect. We can therefore say that areas with persistently higher wages seem to see more transitions, but not that short-term increases in wages within the same area have the same effect.
Figure 5. Occupational mobility and outside job market opportunities

Note: All estimates adjusted for differences in the demographic composition of the local NHS workforce. Details of the regression specifications used are available in the technical appendix. The error bars represent 95% confidence intervals.
The second hypothesis is that areas with higher wages simply hire more registered staff in general, some of whom are recruited through occupational mobility from clinical support roles. This could be the case if these areas employ more registered staff per support worker, or if turnover is higher (as suggested by Kelly, Stoye and Warner (2022)) and so they need to recruit more new registered clinical professionals to maintain the size of their workforce.
To test this mechanism, we focus on nurse recruitment, as earlier results suggest that this is one of the most important options for former clinical support workers. We estimate the association between the same local labour market characteristics as before and the number of new nurses recruited from any source in the same area each year, relative to the number of clinical support staff already working there. We again strip out national-level trends (this time, in nurse recruitment), but allow comparisons across different areas as well as within the same area over time.
Figure 6 displays these results. As in Table 1, the coefficients should be interpreted as the effect associated with a one-unit increase in the labour market variable (such as a £1 increase in hourly wages) on the outcome variable: here, the number of new nurses recruited each year per 1,000 support staff. Across all areas and the period we consider, the mean of this variable is 22.1.
Figure 6. Occupational mobility and nurse recruitment

Note: Details of the regression specification used are available in the technical appendix. The error bars represent 95% confidence intervals.
The patterns here are similar to those in Table 1. Higher-wage areas hire more nurses in general, relative to their number of support staff. There are no clear relationships with the wage growth or concentration variables. This suggests that part of the explanation for why occupational transitions are more common in higher-wage areas is that trusts in these areas simply hire more nurses in general. Some of those additional, newly hired nurses come through routes from clinical support roles.
Taken together, these results suggest that transitions from clinical support roles into nursing are concentrated in areas with higher-paid job opportunities available outside the NHS. This pattern reflects persistent differences between areas, rather than short-run responses to wage changes within areas. Part, but not all, of this effect can be explained by the fact that these areas simply hire more nurses from all sources. This means that whilst many clinical support workers in more deprived areas have gained training and qualifications through these routes, they have not so far served to close gaps in social mobility between higher- and lower-wage areas.
5. Retention and recruitment
In this section, we discuss what the increased rate of transitions from clinical support roles to registered roles has meant for the composition of new cohorts of registered clinical staff. While changes to who is recruited into registered roles might provoke changes in a whole range of workforce outcomes, we here focus on two: hoped-for benefits for retention and for recruitment in registered roles.
Retention
One important aim of expanding routes for support staff to move into registered roles is the hypothesis that this could improve retention. If nurses and allied health professionals recruited from among support staff come from the local community and are already very familiar with the hospital environment, they may be more likely to stay in the role for longer.4
Figure 7 shows that there is some evidence of this: by 2024, the retention rate of registered staff who had joined in 2014 was nearly 10 percentage points higher for staff who had joined after an occupational transition than for those who joined the occupation directly. This does not necessarily mean that it is the experience of having worked in a clinical support role that is causing better retention – it could equally be the case that occupational transitions attract a type of person who would remain in a job for longer, whichever their route into the profession. But whatever the driver behind this pattern, it would suggest that it is not just staff who benefit from these transitions via higher pay, more credentials and a role with greater responsibilities, but also NHS trusts, which could see reduced turnover in registered clinical roles.
Figure 7. Retention rates for registered staff, recruited directly or through transition from another NHS occupation group

Note: Cohorts of registered clinical staff first seen in their role in the relevant year.
However, it is not obvious that more recent cohorts will show exactly the same behaviour as earlier ones, in light of the expansion of newer routes discussed above. Early evidence on retention for the 2022 cohort of new registered clinical staff suggests there has been little difference in retention rates to date by recruitment source. With this cohort still being very new in their roles, this evidence is far from conclusive and we cannot yet tell what the longer-term effects will be. But it remains an open question whether some of the benefits accruing to employers from occupational transitions in the early part of our study period necessarily ‘scale up’ when these transitions become much more common, and are taken up by staff with potentially quite different characteristics from those in earlier cohorts.
Recruitment
Increasing rates of occupational transitions have also changed the composition of new cohorts of staff in registered professions. In Figure 8, we look at cohorts of new nurses and allied health professionals and ask what share previously held a clinical support role in the NHS.
Figure 8. Share of new nursing and allied health professional cohorts who join from other NHS occupations, 2012–24

Note: Clinical support workers include healthcare assistants, support workers, and any other non-registered support staff in patient-facing roles. New nursing and allied health professions cohorts defined as those first seen in those roles in the relevant year.
The graph shows that this share has been rising across successive cohorts of new nurses: whereas around 4% of nurses starting their career in 2012 came from clinical support roles, 12 years later that share had more than tripled (to 16%). The share of nurses recruited from other occupations in the NHS such as midwives and allied health professionals – which are typically lateral rather than upward transitions (at least in terms of pay) – is lower in the more recent years, and if anything has fallen over time.
This rise in nurses joining from clinical support roles has not happened spontaneously, but has been the result of an explicit and ongoing policy effort to establish more routes for this type of occupational mobility. Healthcare assistants and nursing assistants currently undertaking degree apprenticeships and nursing associate courses (Figure 9) will add to the number of transitions in future years, most of which are intended to be existing support staff (Royal College of Nursing, 2025). New routes have been aimed at nursing roles specifically, rather than registered clinical roles in general.
Figure 9. Number of new starters in selected training programmes, 2012–24
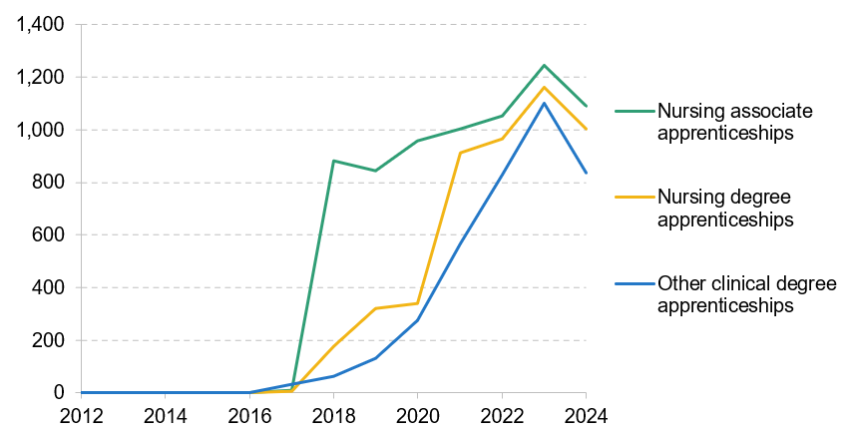
The share of allied health professionals recruited from clinical support roles – which was higher than for nurses in 2012 – has remained roughly constant at around 10% between 2012 and 2024. Nursing is also a much bigger staff group in the acute and community sectors than allied health professionals, even though the latter groups together a range of diverse professions. This means that, even for a similar share of allied health professionals and nurses recruited from clinical support roles, the number of transitions to nursing will be much larger.
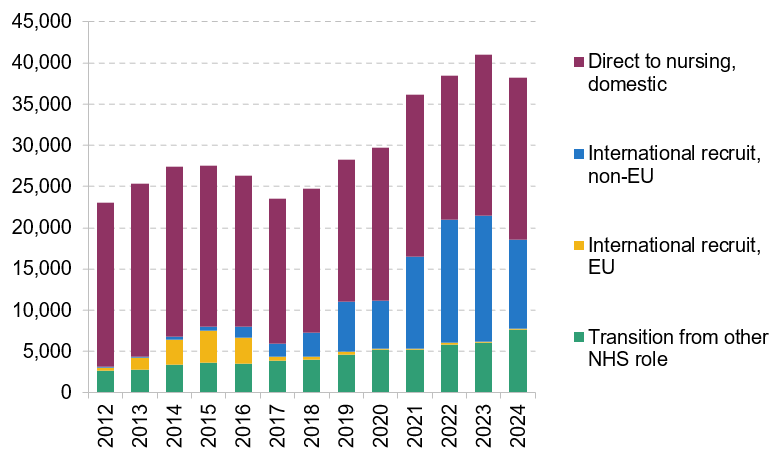
The rise in transitions from clinical support roles into nursing has come amid significant wider shifts in the sources of nurse recruitment into the NHS since the early 2010s. Figure 10 shows that the share of nurses joining from EU countries peaked in 2015 at 14% of the cohort (or 4,000), and almost no new nurses were recruited from the EU after the Brexit referendum. In contrast, international recruitment from outside the EU rose sharply, peaking in 2023 at 15,000 nurses (37% of the cohort). In recent years, occupational mobility has accounted for around half as many new nurses as international recruitment.
Figure 10. Recruitment sources by new nursing cohort, 2012–24
6. Conclusions
In this report, we consider the patterns and extent of occupational transitions within the NHS. We find that clinical support workers are most likely to change occupation, and that the share doing so has doubled in the past decade. The biggest increase has been in transitions to nursing, where the share of clinical support staff moving into registered nursing within four years has tripled. This shift reflects policy efforts to expand routes into nursing from the mid 2010s onwards, through the nursing associate and nursing degree apprenticeship programmes. It also coincides with the previous government’s 2019 commitment to employ 50,000 more nurses by 2024.
Evidence suggests that transitions from clinical support roles into nursing will remain an increasingly important feature of NHS careers. Large recent intakes of apprentice nurses will soon qualify, and the NHS 10-Year Plan pledges an additional 2,000 apprenticeships over the next three years. These expansions aim to create progression opportunities for staff who might otherwise lack them, promote social mobility in disadvantaged areas, and improve recruitment and retention in registered roles. However, achieving these goals depends on the incentives trusts face to offer such opportunities and on who takes them up.
For programmes that help facilitate occupational transitions to succeed, it is important to understand the incentives trusts have to take them up. Offering routes into registered professions, such as nursing apprenticeships, can carry substantial costs for trusts. For example, while the apprenticeship levy may cover the training portion of the nurse degree apprenticeship, trusts must fund the costs of backfilling the apprentice’s role. Trusts will therefore weigh these costs against the potential benefits.
The variation we show in the rates of occupational transitions across the country and by trust type highlights how incentives to offer routes to transition can differ. Trusts that typically find it harder to recruit – such as mental health & learning disability trusts, or those in areas where wages are high outside the NHS – are also those more likely to offer these pathways. By contrast, trusts that face lower levels of competition often find that there are less costly ways to fill vacancies. So far, this has meant opportunities are concentrated in wealthier areas, limiting their impact on reducing social mobility gaps.
Improved post-qualification retention is one potential benefit of offering routes to registered professions, and has been used as part of the rationale for expanding these pathways (NHS Health Education East of England, 2014). We find that early cohorts recruited through occupational transitions have indeed had higher retention rates than direct recruits, but that this difference may be closing as the composition of those taking up training pathways changes. Further research would be needed to determine the causes of these differences in retention, but a continuation of this trend may make trusts less willing to promote these routes or more selective over who they offer them to.
Future patterns and growth in occupational transitions will depend on trusts’ financial constraints and incentives, as well as the willingness of staff members to take them up. In the last parliament, there was a push to increase the number of nurses, but current budgetary constraints could limit trusts’ ability to fund pathways into registered professions or to recruit clinical support workers who could be the nurse apprentices of the future. Looking ahead, the 10-Year Plan commits not just to expanding apprenticeships, but to ‘prioritising areas with the greatest need’. How these areas of need are defined will determine the appropriate policy design. As the NHS considers its new 10-year workforce plan, policymakers should be clear about what these routes are intended to achieve – for individual staff members, for the teams they join and for broader social goals.
Technical appendix
Definitions of NHS occupational groups
The seven occupational groups within the NHS that we use are defined in the table below. Further details on the occupation codes referenced here are available in the NHS Occupation Code Manual.5
Occupation group | Definition | Examples |
Nurses and health visitors | Nurse learners, and all registered nursing roles listed in the N matrix of the NHS Occupation Code Manual (excluding midwives) | Registered nurses |
Midwifery | Midwives | Midwives |
Healthcare scientists | All qualified and trainee healthcare science staff, as listed in the U matrix of the NHS Occupation Code Manual | Biomedical scientists |
Allied health professionals | All qualified and trainee scientific, therapeutic and technical staff, as listed in the S matrix of the NHS Occupation Code Manual | Occupational therapists |
Administration and estates | All administration and estates staff, as listed in the G matrix of the NHS Occupation Code Manual | Clerical and administrative staff |
Ambulance | All registered ambulance staff, as listed in the A matrix of the NHS Occupation Code Manual | Paramedics |
Clinical support staff | Healthcare assistants (HCAs); support workers; all support to registered and qualified clinical staff not mentioned above | Nursing assistants |
Definitions of outside labour market variables
We use data from the Annual Survey of Hours and Earnings (ASHE) and the Business Structure Database (BSD) to construct measures of how employment options outside of the NHS vary across the country and over time for healthcare support workers. The measures we construct are defined in the table below.
Labour market variable | Definition |
Pay in the low-paid labour market | 25th percentile hourly pay in the Travel to Work Area (by workplace location), excluding NHS jobs |
Pay for women in the low-paid labour market | 25th percentile hourly pay for women in the Travel to Work Area (by workplace location), excluding NHS jobs |
Wage growth over the last year for the average low-paid worker | Median real wage growth over one year, for employees at or below the 25th percentile of the wage distribution in the first period |
Wage growth over the last four years for the average low-paid worker | Median real wage growth over four years, for employees at or below the 25th percentile of the wage distribution in the first period |
Concentration of employers | Herfindahl–Hirschman Index (HHI) of the local labour market, excluding NHS employers |
Methodology
Our primary analysis in Section 3 uses multivariate regression at the individual level. Our outcome of interest is , a dummy variable for whether individual who is in a clinical support role at time , in local area , is next seen in the NHS Electronic Staff Record in a different occupation group, subject to the exclusions outlined in Section 2. Our regression specification is
where is the labour market variable of interest, measured at the workplace Travel to Work Area annual level, are individual characteristics (age, gender, ethnicity) and are period fixed effects. The two-way fixed effects specification (presented in red in Figure 5) also includes area fixed effects . Standard errors are clustered at the Travel to Work Area level.
We also present regression analysis at the area level (the series shown in blue in Figure 6). Our specification is
where is the rate of nurse recruitment per support staff member in area at time , and other variables are as defined previously.
References
Department of Health and Social Care, 2020. National recruitment campaign for paramedics, radiographers and nurses begins. https://www.gov.uk/government/news/national-recruitment-campaign-for-paramedics-radiographers-and-nurses-begins.
Department of Health and Social Care, 2025. Fit for the future: 10 Year Health Plan for England. https://assets.publishing.service.gov.uk/media/6888a0b1a11f859994409147/fit-for-the-future-10-year-health-plan-for-england.pdf.
Forsythe, E., 2023. Occupational job ladders within and between firms. IZA Discussion Paper 16682, https://docs.iza.org/dp16682.pdf.
Gilburt, H. and Mallorie, S. 2024. Mental health 360: workforce. The King’s Fund, https://www.kingsfund.org.uk/insight-and-analysis/long-reads/mental-health-360-workforce.
Kelly, E., Shembavnekar, N., Sameen, H. and Bazeer, N. 2022. Lower paid NHS and social care staff turnover. The Health Foundation, https://www.health.org.uk/reports-and-analysis/analysis/lower-paid-nhs-and-social-care-staff-turnover.
Kelly, E., Stoye, G. and Warner, M., 2022. Factors associated with staff retention in the NHS acute sector. Institute for Fiscal Studies, https://ifs.org.uk/publications/factors-associated-staff-retention-nhs-acute-sector.
Kessler, I., Steils, N., Esser, A. and Grant, D., 2021. Understanding career development and progression from a healthcare support worker perspective. British Journal of Healthcare Assistants, 15(11), 526–31, https://doi.org/10.12968/bjha.2021.15.11.526.
Longhi, S. and Taylor, M., 2013. Occupational change and mobility among employed and unemployed job seekers. Scottish Journal of Political Economy, 60(1), 71–100, https://doi.org/10.1111/sjpe.12003.
NHS Digital, 2023. NHS workforce. https://www.ethnicity-facts-figures.service.gov.uk/workforce-and-business/workforce-diversity/nhs-workforce/latest/#by-ethnicity-professionally-qualified-clinical-staff.
NHS Employers, 2024a. Apprenticeships in the NHS. https://www.nhsemployers.org/publications/apprenticeships-nhs.
NHS Employers, 2024b. Staff development pathways. https://www.nhsemployers.org/publications/staff-development-pathways.
NHS Health Education East of England, 2014. Benefits of apprenticeships within the NHS. https://www.hee.nhs.uk/sites/default/files/documents/Benefits%20of%20Apprenticeships%20within%20the%20NHS%20-%20Final_0.pdf.
O’Driscoll, C., Azmoodeh, K., Rana, R. and Hardy, G. 2024. The identity of clinical associates in psychology: a cross sectional, national survey. BMC Medical Education, 24(1), 825, https://doi.org/10.1186/s12909-024-05802-7.
Royal College of Nursing, 2025. Career paths for Nursing Support Workers. https://www.rcn.org.uk/professional-development/your-career/hca/career-paths-for-hcas.
Shembavnekar, N. and Kelly, E., 2023. Retaining NHS nurses: what do trends in staff turnover tell us? The Health Foundation, https://www.health.org.uk/reports-and-analysis/analysis/retaining-nhs-nurses-what-do-trends-in-staff-turnover-tell-us.
Stoye, G. and Warner, M., 2024. Progression of nurses within the NHS. Institute for Fiscal Studies, https://ifs.org.uk/publications/progression-nurses-within-nhs.
University Alliance, 2025. An exploration of barriers and enablers to the expansion of healthcare degree apprenticeships. https://www.unialliance.ac.uk/wp-content/uploads/2025/02/An-exploration-of-barriers-and-enablers-to-the-expansion-of-healthcare-degree-apprenticeships-UoD-and-UA-repor.pdf.
Warner, M., Kessler, I., Manthorpe, J. and Stoye, G., 2023. Patterns of employment amongst nursing associates: evidence from the Electronic Staff Record. https://kclpure.kcl.ac.uk/ws/portalfiles/portal/197842150/Warner_et_al_2023_Patterns_of_Employment_amongst_Nursing_Associates_ESR_Report.pdf.
Data
Office for National Statistics. (2025). Annual Survey of Hours and Earnings, 1997-2025: Secure Access. [data collection]. 27th Edition. UK Data Service. SN: 6689, DOI: http://doi.org/10.5255/UKDA-SN-6689-27.
Office for National Statistics. (2024). Business Structure Database, 1997-2023: Secure Access. [data collection]. 16th Edition. UK Data Service. SN: 6697, DOI: http://doi.org/10.5255/UKDA-SN-6697-16.
NHS Business Services Authority. (2025). Electronic Staff Record (ESR) [administrative data system]. NHSBSA NHS Workforce Services.
Acknowledgements
This research is funded by the National Institute for Health and Care Research (NIHR) Policy Research Programme, through the Policy Research Unit in Health and Social Care Workforce, NIHR206121. The authors also acknowledge financial support from the UK Economic and Social Research Council (ESRC) through the Centre for Microeconomic Analysis of Public Policy at IFS (ES/Z504634/1). Elaine Kelly acknowledges financial support from the Health Foundation. The authors thank the Department of Health and Social Care (DHSC) for access to data from the NHS Electronic Staff Record (ESR). Figures published using the ESR may be different from the official workforce statistics published by NHS England. The views expressed are those of the authors and not necessarily those of the NIHR, the DHSC or the ESRC. Some components of this work were undertaken in the Office for National Statistics (ONS) Secure Research Service using data from the ONS and other owners, which does not imply the endorsement of the ONS or other data owners.
Endnotes
Authors

Olly Harvey-Rich
Olly joined the IFS in 2024 and works in the Healthcare sector.

Elaine Kelly
Elaine works in the Public Finance and Pensions sector and she joined the IFS in 2009 and became a member of the research staff in 2011.

Isabel Stockton
Isabel works in the Healthcare sector, and on the public finances. Their research focuses on retaining and developing the NHS workforce.
More from IFS
Understand this issue



Policy analysis



Academic research


