
Downloads
Download the report as a PDF
PDF | 1.01 MB
Executive summary
Sure Start was the first large government initiative to provide area-based holistic support to families with children under the age of 5 in England. It did so through a network of ‘one-stop shops’, which brought together a range of services to support local families with the aim of enhancing the development and life chances of children under 5. These services included health services, parenting support, early learning and childcare, and parental employment support.
Introduced in 1999, Sure Start initially targeted highly disadvantaged neighbourhoods. Five years later, the 10-Year Strategy for Childcare called for ‘a Children’s Centre in every community’, transforming the initiative into a universal service and growing the network to over 3,000 centres by 2010. At its peak in 2009–10, Sure Start accounted for £2.7 billion of public spending (in 2023–24 prices), around 30% of overall spending on programmes for the under-5s. But in the decade since, the context has been one of funding cuts, consolidation and centre closures, with funding falling by almost two-thirds by 2017–18.
The introduction of the Family Hubs and Start for Life programme in 2022–23 – which also seeks to join up family support services, though for children aged 0–19 and not necessarily all within an actual centre – means that understanding whether, for which children and in which situations integrated service provision is effective remains an important and topical policy issue.
This report brings together the findings of a comprehensive programme of work that IFS has led on the short- and medium-term impacts of Sure Start on children’s outcomes. At the time this research started, there was little evidence on whether Sure Start had benefited children, especially beyond early childhood. Using a robust evaluation methodology and a suite of administrative datasets, this research produced estimates of the impact of having had access to a Sure Start centre between ages 0 and 4 on a wide range of outcomes, including educational attainment, hospitalisations, youth offending, special educational needs and interactions with children’s social care. For most outcomes, we trace out impacts on outcomes from early childhood through adolescence, so well beyond when children were eligible to access the centre. This capstone report brings these results together and produces a comprehensive cost–benefit analysis of the programme.
An important feature of the research is that, across outcomes, it estimates the causal impact of Sure Start centres on the outcomes of children who ‘had access’ to a centre in their early years relative to those who did not. This approach is highly policy-relevant for a programme such as Sure Start whose services were open to all within a community. But it requires defining what having ‘access’ or not means. For most outcomes, we define access as living within a pram-pushing distance of 2.5 kilometres of a centre. For hospitalisations, the data are such that we must use another definition, which is the number of centres within a local authority (per 1,000 children aged 0–4). Across both of these definitions of ‘access’, our results speak to the effects of expanding Sure Start provision to give more families and children access to the programme.
Sure Start benefited children and young people’s health and education
The initial aim of Sure Start was to improve the health and life chances of young children, with a focus on promoting ‘the physical, intellectual and social development of the children served’ (HM Treasury, 1998). The effect of Sure Start on outcomes that can be clearly linked to these aims, such as educational attainment in school and hospitalisations, was overwhelmingly positive.
- Access to a Sure Start centre between the ages of 0 and 4 significantly improved the educational achievement of children, with benefits lasting at least until GCSEs (age 16). Children with access to Sure Start – defined as those who lived within 2.5km of a Sure Start centre – performed significantly better in assessments at ages 7, 11 and 16. Exposure to Sure Start also increased the proportion of children meeting the common GCSE benchmark of five GCSEs at grades A*–C by 0.9 percentage points, an increase of around 2%.
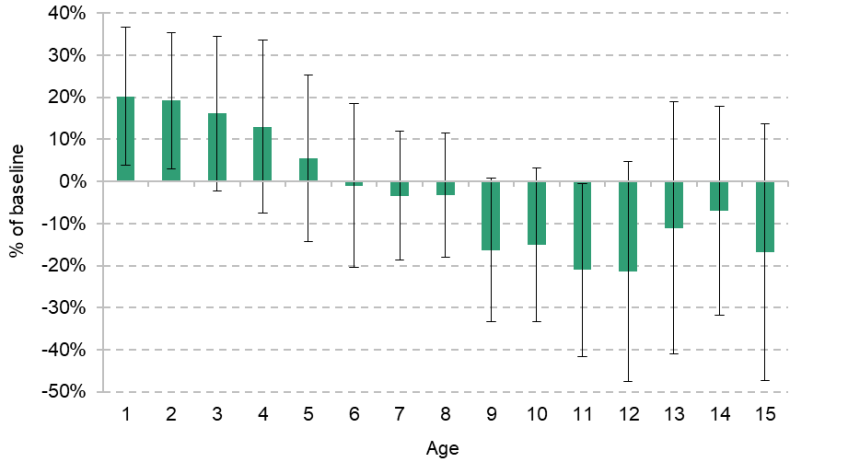
Figure ES.1. Effect of Sure Start on attainment by age
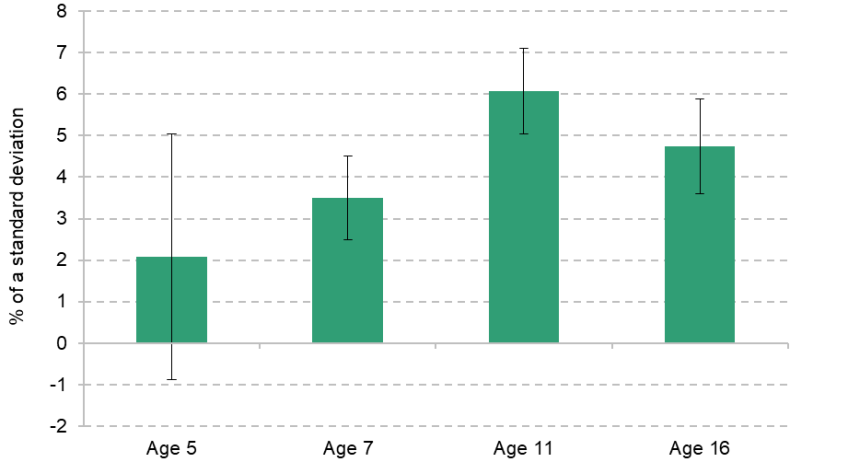
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
- Greater Sure Start coverage (as measured by the number of centres per 1,000 children under 5 in a local authority) substantially reduced hospitalisations during childhood and adolescence. While hospitalisations increased by 10% of the baseline at age 1, they fell by 8.5% of their baseline by age 15 (the final age we study). At a national level, this means that at its peak Sure Start led to an additional 6,700 hospitalisations of 1-year-olds each year, but averted over 13,150 hospitalisations of 11- to 15-year-olds annually.
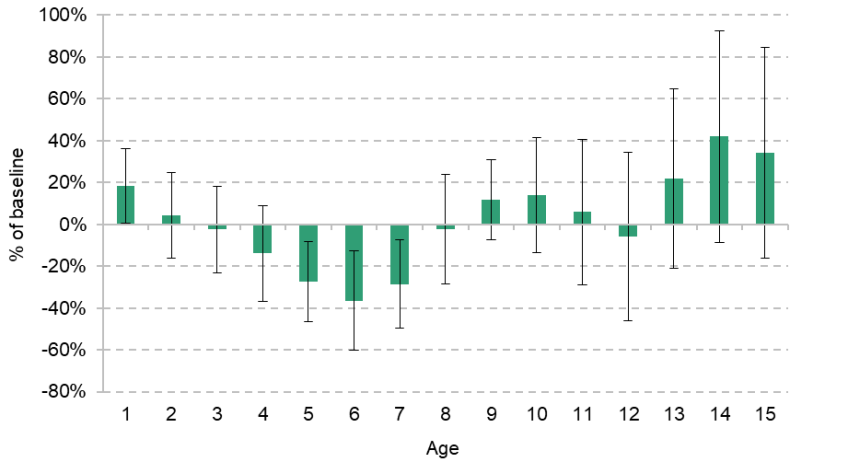
Figure ES.2. Effect of Sure Start on the probability of hospitalisation by age

Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
Sure Start had mixed impacts on children’s socio-emotional and behavioural outcomes
The Sure Start offer could have affected children’s socio-emotional and behavioural development through a number of channels: by providing direct care (e.g. through early education and childcare), by supporting family functioning and the home environment, and/or by changing peer groups. While the aim of Sure Start was to improve children’s well-being, some channels may have led to a positive impact while others may have had a negative impact.
In this report, we study a range of outcomes, some of which are strongly related to socio-emotional and behavioural development. These results suggest that Sure Start had clear benefits in reducing children’s internalising behaviours, such as depression and anxiety disorders, and this is backed up by analysis of young people’s self-reported mental health. However, effects on externalising behaviours, such as conduct disorders, aggression and violence, are much less clear-cut.
- Children who had access to Sure Start in their early years had lower internalising behaviours, such as depressive and anxiety disorders, in their teenage years. Young people who had greater access to Sure Start in their early years reported half as many internalising difficulties as their siblings with less access to Sure Start. Moreover, Sure Start also reduced hospitalisations for mental-health-related causes at ages 12–14, again by around 50% of their baseline.
- On the other hand, we find no significant impact of Sure Start on self-reported externalising behaviours in young people. We do find evidence that Sure Start decreased absences from school, with 15-year-olds who had early access to Sure Start missing 15% fewer school days for unauthorised reasons than their peers. But effects on crime were more ambiguous: children who had more access to Sure Start growing up were more likely to have a criminal record by age 16, driven by an 11% increase in cautions (a 6% reduction in more serious criminal convictions was not statistically significant).
Impacts of Sure Start were remarkably long lasting
Sure Start centres offered services for families with under-5s, but the positive effects of the programme stretched well beyond early childhood and at least into adolescence. Sure Start generated improvements during adolescence in educational attainment and behaviour in school, and reductions in hospitalisations and the number of children receiving support for special educational needs at the same ages. In the case of educational attainment and behaviour in school, the effects were larger than at some earlier points in childhood.
The age profile of impacts of Sure Start across outcomes points to at least four possible – and non-mutually-exclusive – channels through which Sure Start may have been effective.
- Capabilities developed in early childhood helped beget later capabilities. For example, at age 5, Sure Start improved the dimensions of school readiness – communication & language and problem-solving dimensions – that are most closely related to later English and maths competency. These early benefits may have made the acquisition of later skills easier, leading to the effects on test scores through primary and secondary school.
- Sure Start services, which partly focused on enriching children’s home environments, may have generated sustained changes in the child’s family environment. While this research does not generate direct evidence of impacts on the home environment, Sure Start significantly reduced the number of days of primary school missed for unauthorised absences, which tend to reflect parental decisions. It also reduced the number of hospitalisations for external causes, which include injuries and poisonings, likely reflecting improved safety in the home environment. Earlier evaluations of Sure Start found evidence of an improvement in family functioning.
- Sure Start may have helped detect issues early on and prevent them from becoming more difficult (and costly) to solve later on. For example, the reductions in hospitalisations that Sure Start led to in childhood were, in part, driven by a decrease in hospitalisations for ‘preventable’ hospitalisations, such as those where serious illness may have been prevented by early intervention.
- Sure Start may have changed families’ relationship to services, making them more visible to service providers and/or more willing to seek support. While Sure Start reduced the proportion of children receiving support for special educational needs (SEN) at ages 7, 11 and 16, SEN support actually increased at age 5 for those who had early access to Sure Start.
Sure Start was not a ‘silver bullet’
While we find evidence that Sure Start promoted several dimensions of children’s capabilities, our results also suggest that light-touch universal early years services cannot on their own address all challenges that children and young people face. While integrated early years services can benefit children’s lives in a long-lasting way, it is unrealistic to expect that early years services will ever completely replace the need for later, more specialised interventions. In particular, we find that early access to Sure Start had few impacts on the most intensive services.
- While access to Sure Start reduced the share of children with SEN Support plans in later primary and secondary school, we find no impacts on the support received for more serious needs via Education, Health and Care plans.
- Access to Sure Start had no significant effect on the number of children spending time as a Child Looked After (CLA) between ages 7 and 15. Children in care during late primary school (ages 7–11) did spend around 11% less time being looked after if they had access to Sure Start during the first five years of life, but social care contact among secondary school pupils who had had access to Sure Start was often higher (though not statistically significantly so).
- While there is some evidence that early access to Sure Start reduced school exclusions between 14 and 16, these results are not statistically significant. Similarly, Sure Start seems to have had a negative effect on convictions and custodial sentences by age 16, but we cannot rule out that there was in fact no real impact.
The benefits of Sure Start were widespread, but some groups were more strongly affected
The positive effects of Sure Start were spread relatively evenly across different groups, suggesting that the fact that Sure Start services were accessible to all families in the community was important for the outcomes generated. But we do find evidence in some cases that Sure Start reduced inequalities between groups.
- The health effects of Sure Start were more strongly concentrated among children from disadvantaged neighbourhoods. In the education system, Sure Start had benefits on test scores for all children from ages 7 to 16, regardless of eligibility for free school meals, but at age 7 these are significantly larger for children eligible for free school meals.
- Sure Start also increased youth cautions by more for young people who were eligible for free school meals.
- Both boys and girls benefited from Sure Start’s effects on educational outcomes, and there were no differences by gender in the programme’s effects on crime. However, Sure Start’s effects on hospitalisations at older ages were driven by a large reduction in hospitalisations for boys, particularly for accidents and injuries.
- The educational benefits of Sure Start were much stronger for children from non-White ethnic backgrounds, except at GCSE (where impacts were driven by benefits for White young people). Similarly, effects on criminal behaviour were often larger for young people from non-White backgrounds, with both a bigger increase in cautions and a bigger decline in custodial sentences.
Long-run benefits are likely to significantly exceed the costs
By its peak in 2010, total spending on Sure Start was around £2.7 billion in 2023–24 prices, including both day-to-day spending and capital costs. However, the effects outlined in this report are associated with significant financial benefits, both for the government and for the children and families who attended. These come from reduced costs to the government for services at later ages that are not needed, increased earnings for attendees, and increased tax revenue stemming from higher earnings.
Attaching a financial value to these benefits involves considerable uncertainty and quite a few assumptions. We need to make assumptions about where these benefits were felt, how long they lasted, and how they relate to later outcomes such as employment and earnings. We also need to project their financial value over a child’s lifetime, and discount it back to the present day (for which we use the ‘Green Book’ recommended discount rate of 3.5%). The numbers in Table ES.1 should therefore be read as giving a sense of the scale of costs and benefits of Sure Start, rather than as a precise estimate of exactly how those numbers line up.
Table ES.1. Costs and benefits of Sure Start
Costs | Value |
Up-front cost of Sure Start per cohort | £2.7bn |
Benefits | Central estimate |
Government: reduction in later spending for the government | £0.6bn |
Government: increased tax income | £1.9bn |
Total benefits to government | £2.4bn |
Individuals: increased earnings and other private costs/benefits | £3.1bn |
Total benefits | £5.5bn |
Note: Values may not sum due to rounding.
- The effects on medium-term outcomes suggest it is likely that Sure Start generated a range of long-run benefits: the improvements in educational performance are associated with an increase in post-tax earnings of £3.1 billion per cohort over the life cycle (discounted from when the cohort might have attended Sure Start at 3.5%). At today’s basic rate of income tax and rates of National Insurance contributions, this suggests that providing a cohort of children with access to Sure Start could generate an additional £1.9 billion of increased personal tax revenue over their lifetime. Sure Start also directly reduced some of government’s costs through reduced service use (such as fewer hospitalisations and less support required for children with special educational needs), which generated £0.6 billion of savings for the government. Based on the central estimates presented here, these total lifetime benefits – for government and for individual earnings – are equivalent to twice the up-front cost of Sure Start.
- The net cost of Sure Start (i.e. the cost to the government in the long run, when taking into account subsequent savings from reduced service use and expected increases in tax revenue) was less than £300 million, or around 10% of the up-front cost. Comparing this net cost with our central estimate of £3.1 billion in private benefits for children and families implies that for every £1 of net spending, Sure Start may eventually generate around £11 in benefits for the children who attended. Importantly, this measure is highly sensitive to the estimated financial benefits to government (which are driven by our estimates of earnings impacts projected across a child’s lifetime).
1. Introduction
In 1999, the government introduced the first large initiative in England to provide holistic integrated support to families with children in their early years. The ultimate aim of Sure Start was to enhance the development and life chances of children under the age of 5 by providing holistic support to their families. This was to be achieved by developing a network of ‘one-stop shops’, serving their local communities with a variety of services, including health services, early learning, parenting support and parental employment help.
At its peak in 2009–10, the programme had over 3,000 community-based early years service points across England and accounted for £2.7 billion of public spending across current and capital spending (in 2023–24 prices), or around 30% of overall spending on programmes for the under-5s (Britton, Farquharson and Sibieta, 2019). With the change in government in 2010, funding stopped being ring-fenced and significant spending reductions ensued, with spending 73% lower in 2021–22 than it was in 2009–10 (Fright and Davies, 2023) and at least 1,340 centres having been closed.
Despite the apparent recognition of the benefits of integrated services, relatively little was known about the programme’s impacts at times when crucial decisions were made about the future of the programme. While the programme was expanding, two government-commissioned evaluations of it were conducted to document impacts on short-term child outcomes and family functioning. The National Evaluation of Sure Start (NESS), which focused on the first phase of the programme, Local Programmes, found no impact on children’s cognitive skills but an improvement in parenting (less chaos, improved home learning environment) and children’s health (National Evaluation of Sure Start team, 2010). The second evaluation, the Evaluation of Children’s Centres in England (ECCE), was commissioned in 2010 and focused on Children’s Centres, the second phase of the programme. It found that Children’s Centre service use was correlated with improvements in the early home learning environment and reductions in parent–child dysfunctional interaction, chaotic environments and parental distress (Sammons et al., 2015).
Multifaceted early childhood programmes such as Sure Start have the potential to influence numerous dimensions of children’s environments and their development, both immediately and as they grow older. And because of the preventative nature of many services, the true benefits of the programme may only start to emerge many years after children were eligible for it. Together, this means that a comprehensive evaluation of the effectiveness – and cost-effectiveness – of a programme such as Sure Start must consider multiple outcomes, both in the short and longer term.
This report is the final output of a multi-year programme of work the Institute for Fiscal Studies led to this end. It brings together findings from successive strands of (already published) research and presents a comprehensive cost–benefit analysis of the programme. The methodological strength of this research lies in its ability to trace out Sure Start’s impacts, from early childhood through adolescence, on a large array of outcomes, including educational attainment, hospitalisations, youth offending, special educational needs, school absences, and interactions with children’s social care. As part of drawing together these different strands of research, we have updated our methodology in some cases; an overview of these changes, and the impact that they have on our results, is presented in Box 1.1.
Box 1.1. Changes relative to previous reports
This report covers outcomes covered by Cattan et al. (2021) on hospitalisations, Carneiro, Cattan and Ridpath (2024) on educational outcomes and Carneiro et al. (2024) on behaviour and social care interactions. As part of drawing together these different pieces of analysis, we have implemented some methodological updates since the publication of these reports. This means some estimates in this report are updated from prior reports.
The main methodological change was to the weighting method used to ensure comparability in trends in outcomes between areas that received Sure Start earlier and later. We now use a consistent measure of area-level deprivation, the ward-level Index of Multiple Deprivation from 2000. This is likely to be more reflective of the measures of deprivation used in the allocation of Sure Start centres. Reflecting recent developments in the econometrics literature on difference-in-differences, we have also moved away from weighting areas based on their pre-Sure-Start trends in a relevant outcome. This makes the interpretation of results simpler, as estimates now reflect the effect of Sure Start on children living near a Sure Start centre compared with those in similarly deprived areas not living near a centre, rather than depending on the prior trends in the outcome of interest.
This change means some results have changed relative to previous reports, with particularly large changes in the estimates of effects on criminal behaviour, behaviour in school, and specific effects for children from less deprived backgrounds and for children who attended later Sure Start Children’s Centres. A full description of the changes to the methodology and results can be found in Section A.2 of the appendix.
Applying a common, robust evaluation methodology to a suite of administrative and survey datasets, we estimate the causal impact of Sure Start centres on the outcomes of children who ‘had access’ to a centre in their early years relative to those who did not. This approach is highly policy-relevant for a programme such as Sure Start, whose services were open to all within a community. Our research speaks to the impacts on families and children of choosing to expand – or restrict – access to Sure Start, by opening (or closing) new centres, rather than to the effect of a family’s choice to use those services.
Because we look at such a broad range of outcomes over such a long period of children’s lives, we are able to paint a nuanced picture of how Sure Start affected children’s development. We use theory and wider evidence to suggest how these impacts came about – which Sure Start services might have affected which outcomes, and which aspects of children’s development and environments lie beneath the results that we find. But this is as far as our research can go on the question of mechanisms. Unfortunately, there is a lack of data on how Sure Start services were delivered and used, which limits our ability to firmly tie specific outcomes to specific services. A key lesson for future initiatives in this space, such as Family Hubs, is to build in evaluation from the outset and collect the data that will facilitate this work.
Finally, we bring together all of the outcomes that we study in an overarching cost–benefit analysis. But attaching financial benefits to a complex programme such as Sure Start involves considerable uncertainty and quite a few assumptions. The numbers reported here should therefore be read as giving a sense of the scale of costs and benefits of Sure Start, rather than as a precise estimate of exactly how those numbers line up.
The rest of the report proceeds as follows. Chapter 2 provides a summary of the history of Sure Start and the services it offered. Chapter 3 discusses the mechanisms by which we might expect Sure Start to affect medium-term outcomes. Chapter 4 describes the data and methods we use to identify the causal effect of Sure Start. Chapters 5–8 present our estimates of the effect on Sure Start on education, health, behavioural outcomes and interactions with children’s social care respectively. Chapters 9 and 10 examine whether Sure Start was particularly effective for any specific groups, while Chapter 11 presents a cost–benefit analysis of Sure Start at its peak. Chapter 12 concludes this report.
2. History of Sure Start
2.1 The roll-out of Sure Start
Sure Start Local Programmes
Sure Start was introduced as a cornerstone of the New Labour government’s plan to ameliorate the impact of child poverty and tackle social exclusion of children in deprived areas. Its initial main aim was to improve the health and well-being of young children living in the 20% most deprived areas of England. This was to be achieved by setting up community-based Sure Start Local Programmes (SSLPs) or ‘one-stop shops’ for local families with children under the age of 5. SSLPs were managed by a partnership of health, education, social services and voluntary sectors, and each Local Programme was responsible for working with the community to offer a range of services for young families (Melhuish et al., 2008).
When the programme was first announced, the government set aside three years of funding (1999–2000 to 2001–02) to set up 250 projects in areas with a very high concentration of children under 4 living in poverty. Each project was intended to run for seven to ten years, and, in total, the programme would reach up to 150,000 children (Pugh, 2010).
In January 1999, the newly formed Sure Start Unit (a joint responsibility of the education and health departments) identified 60 ‘trailblazer’ districts that would be invited to submit project proposals. On 9 April 1999, the government announced the first 21 projects to go ahead, with a further 30 announced in July. By November of that year, 15 had opened their doors as Sure Start Local Programmes, across almost all regions of the country.
In 2000, the government announced that it would more than double the programme target, from 250 Local Programmes to 530. In total, the government opened 524 Local Programmes by 2004 (Meadows et al., 2011).
Sure Start Children’s Centres
From 2003, the government shifted its approach to Sure Start, as outlined in two key documents published in 2003 and 2004 (Bouchal and Norris, 2014). The first, Every Child Matters, emphasised the need for joined-up services to improve children’s outcomes and proposed a shift from targeted SSLPs to a universal programme controlled by local authorities and relabelled Children’s Centres. The second, the Ten-Year Childcare Strategy, set out plans to make Children’s Centres part of the government’s drive to increase the quality and availability of childcare for families with young children.
The government’s commitment to create ‘a Children’s Centre in every community’ by 2010 led to a rapid increase in the number of Sure Start Children’s Centres (SSCCs) from 2005 onwards, as shown in Figure 2.1. The roll-out of SSCCs was staged in three phases. Between 2004 and 2006, there would be approximately 800 Phase 1 centres, offering full coverage of the 20% most disadvantaged neighbourhoods. Of these, around 500 would grow out of existing SSLPs (and older initiatives, such as Early Excellence Centres and Neighbourhood Nurseries) while the rest would be new centres.1 In Phase 2, between 2006 and 2008, 1,700 new centres would open in the 30% most disadvantaged neighbourhoods. Finally, Phase 3 of the roll-out would complete the universalisation of the programme, through the opening of another 1,000 centres in the remaining 70% of areas. In the least deprived 30% of areas, it was expected that most of these Children’s Centres would open in refurbished or converted existing facilities as opposed to new buildings (Children, Schools and Families Committee, 2010).
Figure 2.1. Number and budget of Sure Start centres in England
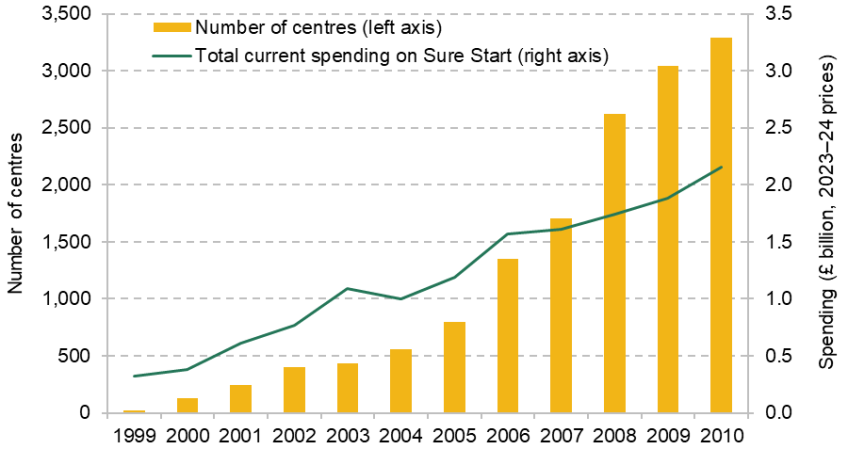
Note: The graph shows the number of centres open at the end of each calendar year. It includes both Sure Start Local Programmes and Sure Start Children’s Centres. Since the treatment of arrangements such as satellite sites was not always consistent, these numbers might not exactly match other data sources. We assume that a Sure Start Children’s Centre opening at the same postcode as a Sure Start Local Programme replaces the SSLP; otherwise, we count both SSLPs and SSCCs between 2003 and 2006, and assume all SSLPs had closed from 2007 onwards. Only current spending is included.
Source: Data on number of centres taken from authors’ calculations using data provided by the Department for Education. Data on Sure Start budget taken from Stewart (2013).
Overall, by 2010 there were 3,290 Children’s Centres in England, with 83% of 4-year-olds living within 2.5 kilometres (or ‘pram-pushing distance’) of a centre.
Figure 2.1 also presents the progression of total non-capital spending on Sure Start throughout the roll-out. This shows that the shift to SSCCs, and the subsequent rapid increase in the number of centres, was not accompanied by anywhere near as rapid an increase in the national budget for Sure Start. In 2003, the last year of Local Programmes, there were 437 centres, and current spending on Sure Start was £1.09 billion (in 2023–24 prices). Over the next seven years, the number of centres grew to be more than seven times larger, while the budget only doubled. This meant that by 2010, the last year of the expansion of Children’s Centres, the average budget per centre was less than a third of what it had been seven years earlier, though with significant variation across centres as former SSLPs maintained much higher budgets than newer centres (National Audit Office, 2009).
2.2 Sure Start services
Sure Start centres integrated a range of early years and family support services, with the aim of providing a ‘one-stop shop’ for families with children under 5. The service offer did change somewhat over the course of the programme’s roll-out, with a greater emphasis on a standardised ‘Core Offer’ and a stronger focus on childcare and parental employment in Children’s Centres. But the emphasis on bringing together a wide range of services for children and their families was constant throughout the programme. Table 2.1 provides an overview of services offered by SSLPs and SSCCs.
Table 2.1. Overview of Sure Start services
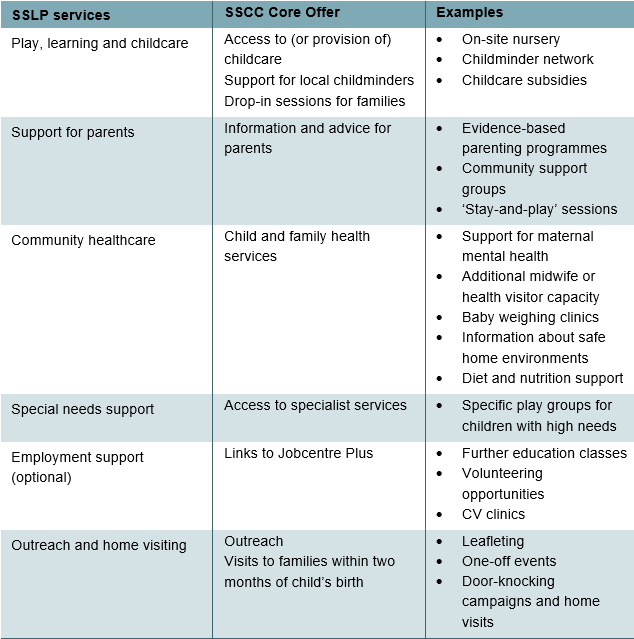
Services in Sure Start Local Programmes2
Sure Start Local Programmes had substantial local discretion over the services they offered. All SSLPs were expected to provide core services in play, learning and childcare; support for parents; community healthcare; outreach and home visiting; and special needs support. SSLPs could also choose to provide additional services, such as classes to support parents’ education and employment or services aimed at teen parents. Within each of these categories, SSLPs chose what services they would provide and how they would deliver this offer. Figure 2.2 summarises how SSLPs allocated their budget to these different service areas in the early 2000s.
Figure 2.2. The share of different activities in SSLP expenditure, 2003–04 to 2004–05
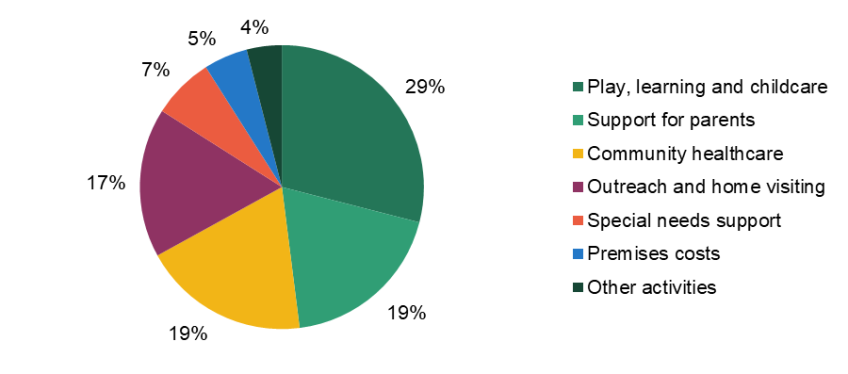
Source: Figure 7 of Meadows et al. (2011).
Services for play, learning and childcare (which excluded funding for the free entitlement) made up the largest share of SSLP spending, and ranged from formal childcare provision to development funding for childminder networks to light-touch, drop-in services such as ‘stay-and-play’ sessions. Community healthcare services offered provision to supplement NHS services – for example, additional services for postnatal depression or breastfeeding support. Outreach and home visiting largely involved efforts to bring families into SSLPs, including leafleting campaigns, one-off open days or community events, and door-knocking campaigns.
The ‘Core Offer’ in Children’s Centres
With the transition from Local Programmes to Sure Start Children’s Centres, the services offered were formalised further in the Sure Start ‘Core Offer’ (Children, Schools and Families Committee, 2010). All Children’s Centres had to provide:
information and advice to parents;
drop-in sessions and activities for parents, carers and children;
outreach and family support services, including visits to all families within two months of birth;
child and family health services, including access to specialist services for those who needed them;
links with Jobcentre Plus for training and employment advice;
support for local childminders and a childminding network.
In addition, Phase 1 and 2 Children’s Centres – those in the 30% most deprived neighbourhoods – were required to offer early education and childcare for at least 10 hours a day, 5 days a week, 48 weeks of the year.
During the early 2010s, the Evaluation of Children’s Centres in England surveyed families registered with Phase 1 and 2 Sure Start Children’s Centres (typically located in the 30% most deprived neighbourhoods and required to deliver the full Core Offer). Overall, Figure 2.3 shows that around 60% of registered families used at least one Sure Start service, rising to 75% of families with a 1-year-old. The most commonly used services were parenting support (43% of families), followed by health services (37% of families).
Figure 2.3. Take-up of Sure Start services in the early 2010s (Phase 1 and 2 centres)
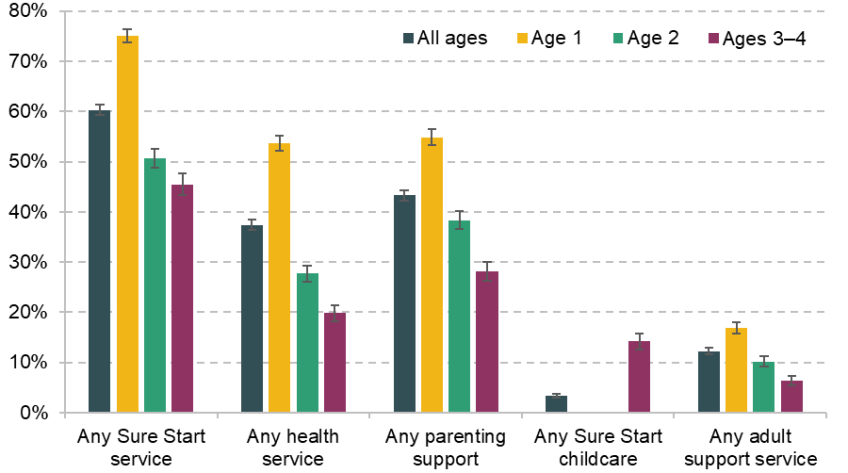
Note: The graph shows the share of families in the ECCE sample that report making use of Sure Start, overall and for each of the four main types of services, by the age of the focus child. This is based on pooling all three waves of ECCE data. Error bars represent 95% confidence intervals.
Source: Figure 1 of Cattan et al. (2025). Original data from Goff et al. (2013).
For all services except childcare, families with younger children were substantially more likely to use Sure Start than those whose children were slightly older. While only a small minority of families used Sure Start childcare services, this included 14% of families with a 3- or 4-year-old (who, at that time, were the only age groups eligible for funded childcare under the ‘free entitlement’ programme).
3. Potential effects on children’s development
In this report, we consider numerous child outcomes, ranging from universal measures (such as performance in national tests) to measures of engagement with specialist services such as children’s social care or special educational needs (SEN) support services. We look broadly across education, health, crime and children’s social care.
In most cases, these outcomes are not themselves measures of children’s development. Rather, they capture the outcomes that are influenced by children’s cognitive development, their social and emotional development, and their health. But these outcomes are also influenced by aspects of the child’s or young person’s environment: the environment at home, the peers that a young person has, and their families’ willingness to engage with services. All of these factors, too, can be influenced by Sure Start.
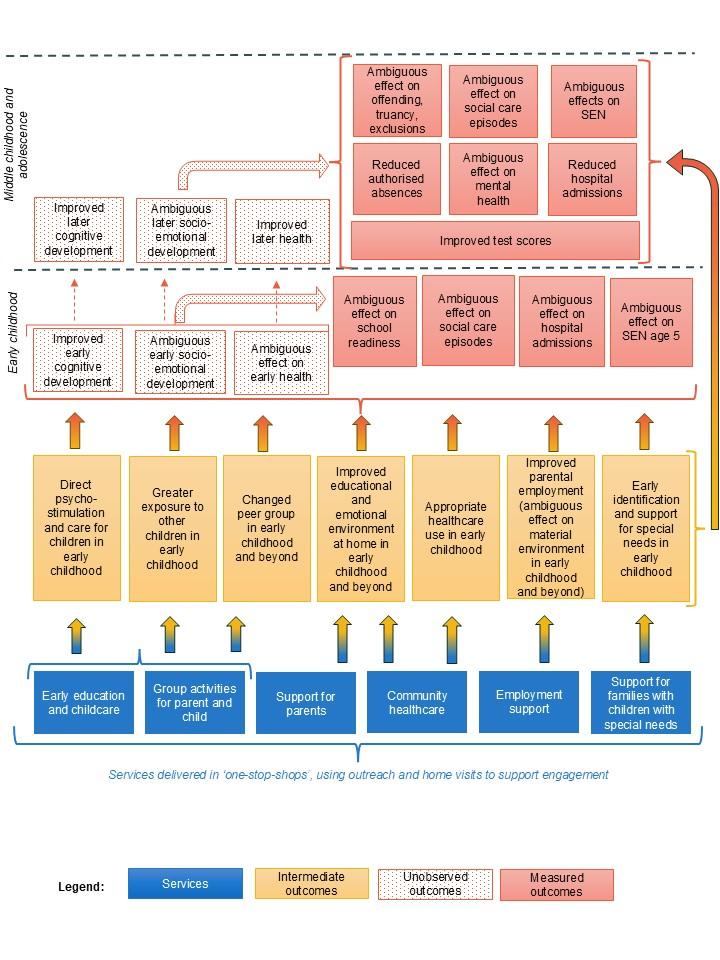
In this chapter, we outline the different channels through which Sure Start might have influenced test scores, hospitalisations, absences, crime and the use of specialist services. We summarise the pathways through which Sure Start services may have affected the outcomes we consider in this evaluation in Figure 3.1.
Figure 3.1. Channels through which Sure Start services may have affected the outcomes considered in this evaluation
3.1 Potential impacts on test scores
Sure Start brought together a range of services aimed at supporting children’s early development. Most directly, early learning and childcare services gave children additional access to a stimulating environment, often with input into learning development from qualified teachers. Raising the take-up and quality of formal childcare in later childhood may have long-lasting benefits for children’s cognitive development, especially for those from disadvantaged backgrounds.
Greater support for parents – especially in the form of evidence-based parenting programmes – may also lead to improvements in the home learning environment. For example, parents with more access to support might have had better mental health themselves, or better information about positive parenting strategies. This in turn can support children’s cognitive and socio-emotional development.
Other Sure Start services might have also had indirect effects on children’s test scores, including through improvements in health (thereby reducing absences), more appropriate support for children with special educational needs, or higher family income (and thus more access to learning support) as employment support helped parents move into paid work. We discuss these channels later in this chapter, when we look at the services that might have affected each of these outcomes. (We explore Sure Start’s impacts on maternal employment in Section A.4 of the appendix, which shows limited effects. We therefore focus more on other channels through which Sure Start could have influenced children’s development in the rest of this chapter.)
Given the range of services that Sure Start offered, we would expect to see positive impacts (if any) on children’s cognitive development and possibly on children’s socio-emotional development in early childhood, which may translate into higher school readiness at age 5 or at least improvements in dimensions of school readiness most related to cognitive development.
These impacts may persist beyond early childhood, both because early skills help beget later skills and because changes in parental behaviours and/or attitudes persist over time. In turn, we would expect these to be reflected in greater academic achievement in primary and secondary school.
3.2 Potential impacts on hospitalisations
Our main measure of children’s health outcomes is admissions to (NHS) hospitals. Of course, hospitalisations capture both children’s health and how they (or their parents) choose to use healthcare. Sure Start could have improved children’s health and so reduced hospitalisations. But Sure Start could also have increased detection of health problems and led to an increase in the share of children seeking medical care. It is therefore not possible to say at the outset what impact Sure Start might have on hospitalisations and whether an increase in hospitalisations is ‘good’ or ‘bad’ news.
To help disentangle these potential channels, in this report we will consider hospitalisations for specific causes: infectious illnesses; accidents and injuries; ‘preventable’ hospitalisations; and – in adolescence – hospitalisations related to mental health. We will also look briefly at self-reported general and mental health among adolescents, using survey data (as opposed to administrative data on hospitalisations).
Across all types of hospitalisations, Sure Start’s impact on engagement with servicesis ambiguous. Greater access to community healthcare services could have provided lower-level care (either directly or through referrals to primary care) and kept children away from hospitals. On the other hand, early screening and detection might have made parents more aware of their child’s need for healthcare, and more willing to seek out medical treatment.
Infectious illnesses
Greater access to Sure Start in the early years could have influenced hospitalisations for infectious illnesses in different ways. Community healthcare services, including better information on safe home environments and on diet, could have reduced children’s exposure to infections. On the other hand, most services at Sure Start took place in groups, with children and their parents meeting and interacting with many other families. This would have increased young children’s exposure to germs and raised the risk of infection, at least in the short term.
However, earlier exposure to infection can also support the development of children’s immune systems, making them more resilient when exposed to infections later on. We would therefore expect an early increase in infections to be followed by a later drop. This profile of short-term increases in infections followed by a decline has been seen in other contexts – for example, in Sweden (van den Berg and Siflinger, 2022) and Denmark (Daysal et al., 2024).
Accidents and injuries
Around three-quarters of hospitalisations for ‘external’ causes relate to injuries; most of the rest are due to poisonings. In the early years especially, a reduction in injuries and poisonings could reflect safer home environments as a result of better information about child-proofing homes.
In later childhood and adolescence, the child’s own behaviour becomes a more important driver of injuries; the most common condition from age 9 onwards is a broken arm. A child with stronger social and emotional development might be less likely to engage in risky behaviours, including both accidents and fights. Indeed, several studies report a correlation between children’s behavioural issues (e.g. hyperactivity and aggressive behaviour) and hospitalisations for injuries (e.g. Hoare and Beattie, 2003).
Finally, Sure Start might have reduced hospitalisations for accidents and injuries by reducing child maltreatment, through better support for parents and/or earlier screening into the children’s social care system. Data on hospitalisations do not usually allow us to distinguish the cause of a particular injury, and so we cannot directly examine hospitalisations where maltreatment contributed.
Preventable conditions
Hospitalisations for ‘preventable’ conditions capture hospitalisations that could have been averted by better care (Blunt, 2013). They include vaccine-preventable conditions such as measles; chronic conditions, such as asthma, that would normally be managed in primary care; and acute but preventable conditions such as gangrene.
Better information and signposting from community healthcare services might have prevented some of these conditions, or helped parents to manage them at home or with a GP. A push for vaccinations would directly reduce the number of vaccine-preventable illnesses, while better information about managing chronic conditions such as asthma might help children and their families to avoid relying on the hospital for acute treatment. In some cases, a referral or screening from Sure Start might have increased families’ use of healthcare services in the short term (e.g. if parents wanted to get a particular condition diagnosed or get initial advice on how to manage it at home).
Mental health
Finally, Sure Start could also have affected hospitalisations for mental health conditions. These are not typically diagnosed or recorded before the end of primary school, so in this report we focus just on mental health-related hospitalisations between ages 12 and 15 (as well as self-reported mental health among a smaller survey-based sample of young people).
The main channel through which Sure Start could have affected mental health is via improvements in social and emotional development. As outlined above, many of the services that Sure Start provided – including positive parenting programmes, support for a safer home environment, support for maternal mental health, and group-based play sessions – could have affected children’s socio-emotional and behavioural development in the early years. These effects might well persist: there is clear evidence that ‘skills beget skills’ and so an early improvement in social and emotional development makes it easier for a child to continue to develop throughout their life (Cunha, Heckman and Schennach, 2010). Moreover, some of Sure Start’s services – such as support for maternal mental health – could have a long-lasting impact on the child’s home environment, feeding a ‘virtuous cycle’ supporting children’s emotional and behavioural health.
3.3 Potential impacts on absences
As highlighted above, one way that Sure Start could have influenced test scores is by reducing absences from school. In this report, we consider impacts on both ‘authorised’ absences – where children have permission from the school to be off – and ‘unauthorised’ absences.
Authorised absences
Around 75% of authorised absences are due to illness; a further 7% are due to medical appointments. This means that reductions in authorised absences can be interpreted as an improvement in children’s health. As we set out above, Sure Start could have reduced illnesses and infections during the school years (by exposing children earlier to illnesses during group-based sessions, and so strengthening their immune systems). We would therefore expect children with access to Sure Start to have fewer authorised absences, particularly in the earliest years of school (when their classmates who had not had access to Sure Start were ‘catching up’ in their exposure to illnesses and infections).
Unauthorised absences
Unsurprisingly, the reasons for unauthorised absences are less well recorded than those for authorised absence. For absences where a reason is recorded, the most common reason is an ‘unauthorised holiday’. These can include term-time family holidays as well as children missing a day or two of school. Unauthorised lateness also counts towards these absences.
Particularly in the earlier years, unauthorised absences usually reflect a parent’s decisions about whether to keep a child home. In this case, a more engaged home environment that places more emphasis on the importance of school might lead to fewer unauthorised absences.
Later, a child or young person might also choose to skip school themselves. Young people with stronger social and emotional development might be less tempted by skipping school. Better results at school might also reduce unauthorised absences, as children and young people feel more engaged in their education.
Peers also play an important role in unauthorised absences. Here, the potential effects of Sure Start are less clear. If young people are more sociable and have stronger peer networks (as a result of better social development), their peers might have more influence over their behaviour. On the other hand, since Sure Start was an area-based intervention, many of a young person’s peers could also have benefited from access to Sure Start. This opens up the possibility of positive peer networks, where young people reinforce one another’s positive decisions.
3.4 Potential impacts on crime and school exclusions
Criminal behaviour among young people is not uncommon in England. Around 10% of young people in our sample had some criminal record by age 16. The vast majority of these had had a ‘caution’, which is a formal warning by police that carries no sanction but remains on a young person’s criminal record.
An improved parent–child relationship and more positive parenting could directly reduce youth offending. Similarly, improvements in children’s development – both cognitive and socio-emotional – could reduce the rate of youth offending. However, while many Sure Start services were targeted towards improving these types of development, there is some evidence that exposure to group childcare services, which Sure Start provided, can lead to worse behavioural outcomes (Baker, Gruber and Milligan, 2008; Fort, Ichino and Zanella, 2016), which could lead to increased youth offending.
Much misbehaviour is driven by peer networks (Gaviria and Raphael, 2001; Carrell and Hoekstra, 2010), and so the effect of Sure Start on peer relationships might play an important role. Sure Start may have increased the influence of young people’s peers (by strengthening friendship networks). This could increase youth offending, or might have a more limited impact if the young person’s peers also benefited from stronger social and emotional development.
A similar set of potential mechanisms apply to school exclusions, where a child or young person is temporarily or permanently excluded from school. According to statistics from the Department for Education (2025), the most common reason for exclusion is persistent disruptive behaviour, followed by verbal abuse of adults and physical assault of other pupils.
3.5 Potential impacts on specialist services
Sure Start could also have influenced the use of specialist services. In this report, we consider two key specialist services for children and young people: support for special educational needs (SEN) and support through the children’s social care system. In both cases, we are only able to observe outcomes once children have aged out of Sure Start and entered the school system.
Special educational needs
Access to Sure Start early in life could directly affect the take-up of services for special educational needs and disabilities (SEND).3 Both SSLPs and SSCCs were required to offer support for children with special educational needs. This included screening services, which would boost rates of detection and diagnosis – and might therefore increase rates of SEN support later on in the schooling years. It could also include early specialist support – for example, with speech and language difficulties. To the extent that these early support services helped to reduce the impact of these underlying special needs, they could reduce the need for SEN support later on.
Children’s social care
Similar mechanisms are at play in the children’s social care system. Increased contact with services early in life would bring opportunities for safeguarding issues to be noticed and flagged. This higher rate of detection could increase social care referrals in the earliest years, while children were attending Sure Start. (Indeed, Anderberg and Olympiou (2023) find evidence of an increase in local-authority-level social care prevalence among under-5s in local authorities with greater access to Sure Start Children’s Centres.) If these children are then ‘on the radar’ for social care services, early detection may also lead to a persistent increase in interactions with children’s social care.
On the other hand, many of Sure Start’s services could have reduced the incidence or severity of safeguarding issues that children are exposed to. For example, evidence-based parenting programmes aim to teach positive parenting strategies, including for discipline and behaviour. This could reduce the incidence of abuse, neglect or maltreatment at home, and therefore reduce the need for children’s social care.
4. Data and methodology
This report summarises a body of work on the causal impact of families having improved access to a Sure Start centre during the first five years of their child’s life on their child’s educational attainment, hospitalisations, special educational needs, behaviour in school and criminal justice settings, and interactions with children’s social care. To do this, we use data on each of these outcomes, and different proxies for access to Sure Start. Different outcomes are measured at different ages, and derive from datasets covering different years, meaning that we do not capture the effect on the same cohorts for every outcome. A full list of the main outcomes considered and the cohorts for which we are able to estimate the effects can be found in Table 4.1.
4.1 Data
The analysis in this report uses data derived from three administrative data sources.
National Pupil Database and linked datasets
For the analysis of the effect of Sure Start on all outcomes besides hospitalisations, we use data from the school census dataset in the National Pupil Database (NPD). This includes data on children’s home postcode in each school year for all pupils in state schools, starting from age 5. We use a child’s address at age 5 as a proxy for their address from ages 0 to 4, when they might have had access to a Sure Start centre.4 The school census also includes a range of additional demographic characteristics, including gender, ethnicity and eligibility for free school meals, which we use to explore whether the impact of exposure to Sure Start differed for different groups. The school census can be directly linked to data on a range of additional outcomes.
Data on educational attainment are also included in the NPD. We use data from school readiness assessments based on the Foundation Stage Profile (FSP) at age 5, as well as data on Key Stage 1, 2 and 4 test scores at ages 7, 11 and 16 respectively. At FSP, we use scores from across all domains of development. At Key Stages 1 and 2, we use combined scores from reading and maths assessments. At Key Stage 4 (GCSE), we combine English, maths and science results. In each case, results are standardised within cohort.
These data also include information on whether students were registered as receiving support for special educational needs at different ages, as well as the level of support they received (i.e. whether they had what is now known as an Education, Health and Care plan). FSP scores started being collected for a subsample of students in academic year 2001–02 and for all students from 2003–04, so for this outcome we are working with a sample of children born from 1997 onwards. For Key Stage 1, 2 and 4 outcomes, we work with a sample of children born from 1990 onwards. The last cohort included in our sample is the cohort of children born in 2007, except for Key Stage 4 results at GCSE level at age 16 for which we only have data for children born up until 2003 (see Table 4.1).
Table 4.1. Cohorts studied by outcome
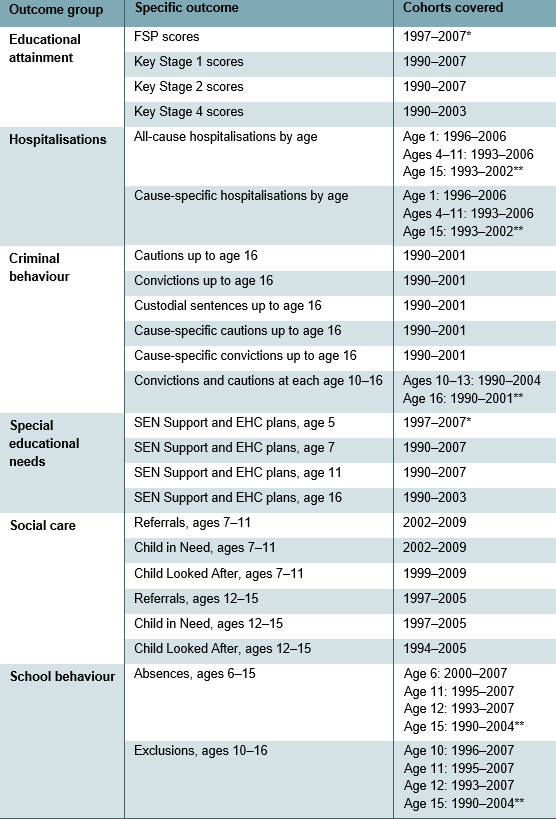
* FSP scores and special educational needs data are for a reduced subsample for the 1997–99 birth cohorts.
** For ages not specified in the table, one earlier year’s set of births are included for outcomes at one year older, and one later year’s set of births are not included.
Data on school-related behaviour are taken from specific datasets within the NPD, which track information on individuals’ absences from school and spells of suspension from school. For absences, this allows us to construct variables indicating what percentage of time in school children miss, both in total and broken down between unauthorised and authorised absences. For both suspensions and permanent exclusions, we combine data on each individual exclusion with information on the total school population from the NPD, taken at each age from 10 to 16, which gives us rates of exclusion and suspension from school.
For criminal behaviour, we use the linked National-Pupil-Database–Ministry-of-Justice data, with which we link the school census to the Police National Computer (PNC). The PNC database includes the criminal history of all children matched to the NPD, covering all recordable offences for which they received formal sanction between 2000 and 2017. We mostly focus specifically on crimes committed up to the age of 16, allowing us to focus solely on the outcomes of children born up to 2001, though at younger ages we can observe more cohorts.
The offences captured in the PNC database include both those for which the offender received a police caution and those for which they received a guilty verdict in a court appearance. For guilty verdicts in court, the PNC database also includes data on severity of sentence received. In order to get a sense of the most severe offences, we categorise sentences into custodial and non-custodial, where a sentence is custodial if it involves detention in a young offender or adult institution. The PNC database also includes data on the specific offence for which individuals were sentenced or cautioned. We group these into broader categories of offences. The most common categories of offence we consider are theft, drug offences, weapons offences and violent crime.5
Finally, for children’s social care, we use data linking the school census to the Children in Need (CIN) and the Children Looked After (CLA) censuses. This allows us to estimate the effect of Sure Start on the number of episodes children have with children’s social care at different levels of severity, and the length of each interaction. The data also record primary need for each spell in care, allowing us to observe whether Sure Start affected different types of need differently. Because of restrictions in the years covered by each census, we observe social care outcomes for younger children and older children based on cohorts that mostly do not overlap, who were mostly exposed to different eras of Sure Start.
Hospitalisations data
We focus on children’s hospitalisations using data from the Hospital Episode Statistics (HES), an administrative dataset tracking all patients using public hospitals in England. Data on inpatient admissions provide information on the admission, discharge, clinical diagnoses and demographics of each patient. These were not linked to the NPD, so we use lower layer super output area (LSOA) at the time of admission as our proxy for where children lived before the age of 5.
Because HES data are not linked to the NPD, we do not have any information on the outcomes – or existence – of children who were not hospitalised. In order to calculate Sure Start’s impacts on the probability of hospitalisation, we therefore collapse the data on admissions at each year of age into ‘cells’ defined by LSOA, gender and quarter of birth. Since close to 90% of these cells have zero admissions (and just 3% have multiple admissions), we define our main outcome of interest as an indicator for whether there is any hospitalisation at a particular age in the LSOA–gender–quarter-of-birth cell.
Data on Sure Start
We use data provided to us by the Department for Education on the exact location and opening date of all Sure Start Local Programmes (SSLPs) and Children’s Centres. We have no information on when Local Programmes closed and hence need to infer it. For SSLPs that match with a Children’s Centre, we assume that the Local Programme closed when the Children’s Centre opened. For other SSLPs, we assume a closure date of December 2006.6 We use this in conjunction with different proxies for where children lived before the age of 5 to generate different definitions of exposure to Sure Start.
4.2 Empirical approaches
Defining access to a Sure Start centre
Sure Start did not have strict catchment areas, but rather aimed to act as ‘one-stop shops’ within ‘pram-pushing distance’ for their local communities. This means that there are many different possible definitions of having access or being exposed to Sure Start.
All outcomes except hospitalisations
For non-hospitalisation outcomes, we consider all families living within a particular small neighbourhood (a lower layer super output area, LSOA)7 as being exposed to Sure Start in a particular year if there was a Sure Start centre within 2.5 kilometres (km) of all postcodes within that LSOA. We define a child/family as having access to Sure Start if, based on their home postcode at age 5 (from the NPD), they lived in an LSOA which had been within 2.5km of a Sure Start centre for at least five years (i.e. since the child was born).
The estimates we derive for these outcomes therefore refer to the average impact of exposure to Sure Start between ages 0 and 4 on the outcomes of all children living within 2.5km of a centre. This parameter is highly policy-relevant because Sure Start was an area-based programme open to all local children and families.
It is worth noting two things about this interpretation. First, not every child who lived near a Sure Start centre would have attended the centre. As a result, the impacts we report are an average of the impacts of the centres on children who used services and children who did not. Children who did not use the services may still have benefited through their interactions with children or families who used the services – though we would anticipate these impacts to be much smaller than any direct impacts from using the services. We do not have data that would allow us to disentangle direct from indirect effects – which is another reason why we focus on estimating the average impacts of Sure Start on the whole of their local communities.
Second, some children who lived more than 2.5km from a centre also attended Sure Start centres, though in much smaller proportions than those living within 2.5km (Goff et al., 2013). As a result, our main estimates should not be considered to represent the difference between living near a Sure Start centre and that centre not existing, but rather the difference between living closer to or further away from a centre. This is the relevant parameter when considering the expansion of an existing programme (such as Sure Start or Family Hubs) in which new centres would increase accessibility for some children/families. In Chapter 11, we spell out what we can learn about the likely effect of actually attending a Sure Start centre from these results.
Hospitalisations
Our data on hospitalisations are not linked to the NPD, and we do not have information on home postcode at age 5. Instead, we observe the family’s LSOA of residence at the time of admission, which could occur at any age between 0 and 15. Given that this is a coarser measure of location, there will be more measurement error if we try to use a precise indicator for the distance between home and the nearest Sure Start centre. We therefore use a different proxy for access to Sure Start, examining the coverage of Sure Start centres in a child’s (lower-tier) local authority (LA) of residence. We define coverage as the number of Sure Start centres per 1,000 children aged 0–4 in the LA district. To arrive at a single treatment measure for each cohort, we average coverage over the first 60 months of life (or over the months leading up to the relevant birthday for outcomes measured earlier (e.g. months 0–11 for outcomes at age 1, months 0–23 for outcomes at age 2, etc.).
This means that our hospitalisation results will present the effect of an additional centre per 1,000 children under 5. This was roughly the average level of coverage by the programme’s peak in 2010.
Estimating the causal effect of access to a Sure Start centre
The Sure Start programme was initially targeted at the most disadvantaged areas of the country, and then gradually rolled out to less and less disadvantaged areas. This means that we cannot simply compare the outcomes of children who had access to a centre with the outcomes of children who did not to estimate the causal impact of Sure Start exposure on children’s outcomes. Doing so could confound the impact of Sure Start with the impact of other pre-existing differences in environments between children who were exposed (and tended to live in more deprived areas) and children who were not (and tended to live in less deprived areas).
To circumvent this challenge and only capture variation in children’s outcomes that can be attributed to exposure to a Sure Start centre, we use an evaluation methodology called difference-in-differences. To understand the intuition behind this methodology, consider a cohort of children residing in an area where a Sure Start centre was located (a ‘treatment area’) who were born just before the centre first opened, and another cohort of children residing in the same location but who turned 5 before the centre was opened and therefore could not benefit from its services.8 Using the difference across cohorts within areas before and after the opening of a centre ensures that our estimates are not contaminated by differences in outcomes across areas that would have occurred even in the absence of Sure Start, such as increases in educational spending across the country over the 2000s.
However, this approach could also pick up any trends in outcomes across cohorts that would have occurred even in the absence of a Sure Start centre opening. We estimate these common national trends from the same cohorts of children residing in areas where Sure Start centres never opened, or only opened much later so that no children in these cohorts were ever exposed to its services (‘comparison areas’). We net off the difference in outcomes over time in comparison areas from the difference in outcomes over time in treatment areas. As long as the trend in outcomes in comparison areas provides a good proxy for what would have happened to outcomes in treatment areas in the absence of a Sure Start centre opening, this should enable us to estimate the causal impact of access to a Sure Start centre on children’s outcomes.
We use this difference-in-differences strategy with both measures of access to Sure Start discussed above. In the case of non-hospitalisation outcomes, where we use living within 2.5km of a Sure Start centre as the treatment measure, we add an additional adjustment: to maximise the comparability of our treatment and comparison areas, instead of treating all comparison areas similarly, we more heavily weight those areas without Sure Start centres that are of a similar level of deprivation to areas with centres, and vice versa. Section A.1 in the appendix presents the technical details of this methodology and discusses the success of this approach in ensuring we are comparing similar areas.
5. Effects on school outcomes
5.1 Educational attainment
Figure 5.1 reports estimates of the effect of access to Sure Start on academic results at ages 5, 7, 11 and 16. In each case, results are reported as a percentage of a standard deviation. This means that in each case, results are scaled according to the distribution of grades in that year. To put this into context, for those born in the first year a Sure Start centre opened in their location of residence, a 1 standard deviation increase in grades in English, maths and science at GCSE would correspond to an improvement of around 2 grades in each subject.
Figure 5.1. Effect of Sure Start on attainment by age
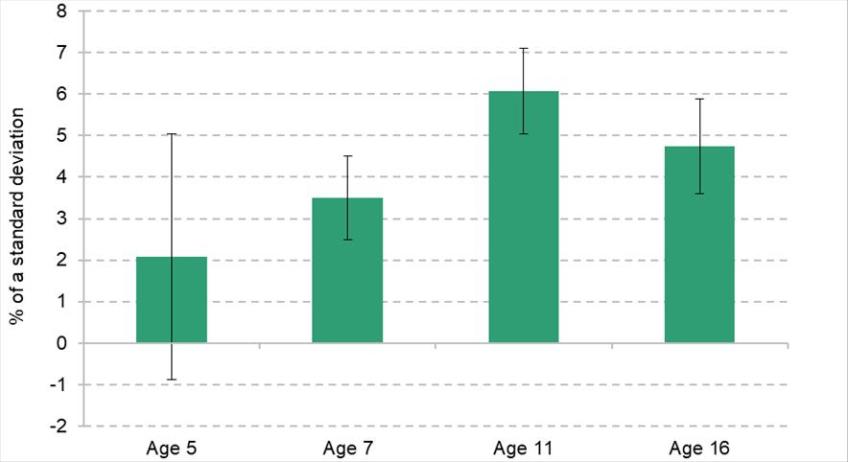
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
The first bar in Figure 5.1 shows that children did not have significantly better aggregate developmental scores at age 5, around the time most children would have stopped being eligible to use Sure Start services.While the effect size is positive at 2.1% of a standard deviation, it is small and statistically insignificant (which means we cannot be confident that the true impact is different from zero).
Two years later, at age 7, students did significantly better in Key Stage 1 assessments because of their exposure to Sure Start – their results are 3.5% of a standard deviation higher than they would have been had they not been exposed to Sure Start. This is even clearer in the results at age 11, where we see an increase of 6.1% of a standard deviation in results in Key Stage 2 exams, the largest we see at any point, and roughly equivalent to the effect of an additional month of learning.9 The effect of Sure Start on school performance is not quite as large at age 16, but is still significant and positive. The improvement of 4.7% of a standard deviation across English, maths and science GCSEs is equal to an increase of 0.1 grades across each of the three subjects.10 We also estimate that access to Sure Start increased the probability of obtaining five A*–C grades at GCSE by 0.9 percentage points.
The lack of effect on aggregate age 5 scores may seem surprising given the relatively large and significant results at later ages. There are a number of possible explanations. First, the sample we have at our disposal to estimate impacts on FSP is smaller than the sample we have for later ages. This could make our results more imprecise. The second, more conceptual reason is that the aggregate FSP score is a composite score reflecting development across seven dimensions, including personal development, language and communication, mathematics and reasoning, knowledge and understanding of the world, physical development and creativity. It may be that Sure Start affected some dimensions more than others, resulting in an insignificant aggregate effect masking some dimensions with larger and smaller effects. We explore whether this is the case by estimating the effect of Sure Start on different domains of school readiness from Foundation Stage Profile tests at age 5.
Figure 5.2 shows the results of this estimation. We see a statistically significant effect on language and communication of over 4% of a standard deviation, and we observe an increase of 3% of a standard deviation for problem solving and reasoning, though it is not quite statistically significant. The effects on other developmental scores across personal development, physical development, and knowledge cannot be statistically distinguished from zero (though there is evidence of a significant increase in scores on the assessment of creativity). Sure Start seems to have affected the more ‘academic’ dimensions of the Foundation Stage Profile scores, which are more predictive of later Key Stage 1 and 2 scores which average achievement in maths and English.
Figure 5.2. Effect of Sure Start on Foundation Stage Profile domains
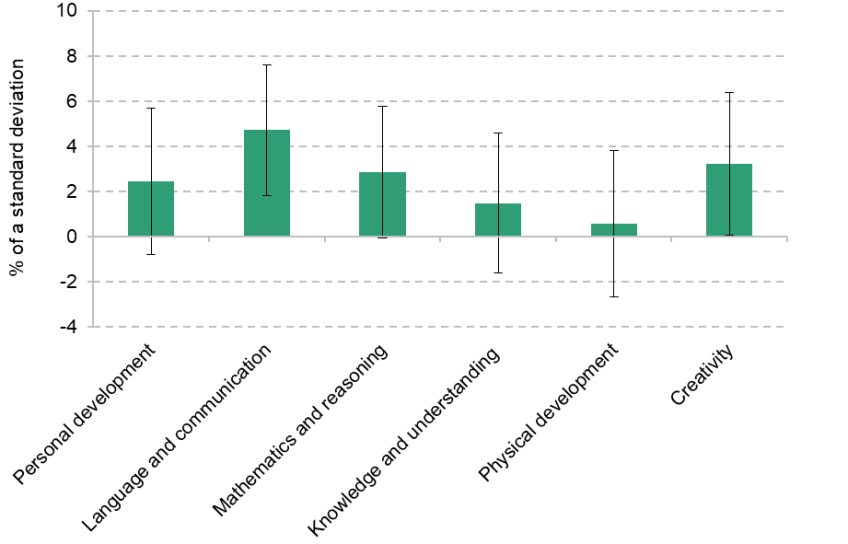
Note: Results represent the difference in developmental scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National Pupil Database.
5.2 Special educational needs
As with academic attainment, we examine the effect of Sure Start on children’s special educational needs (SEN) status at ages 5, 7, 11 and 16. We break down the overall effect into effects for those with SEN Support plans (with typically less severe needs) and for those with Education, Health and Care (EHC) plans (with typically more severe needs).11
Figure 5.3 presents the causal impact of exposure to Sure Start on the probability of students being identified with special educational needs at each age, broken down into the two categories of SEN. This shows that at age 5, students were significantly more likely to have a SEN Support plan (the less severe category) if they were exposed to Sure Start than if they had not been exposed to it. One plausible explanation for this result is that the extra support Sure Start incorporated for those with special educational needs may have helped with detection of additional needs, or simply made it easier for children identified to access support at an earlier age. In other words, it is possible that this is primarily due to an increase in diagnoses of SEN and offering services to children who need them, as opposed to an increase in the proportion of children who have special educational needs.
Figure 5.3. Effect of Sure Start on special educational needs by age
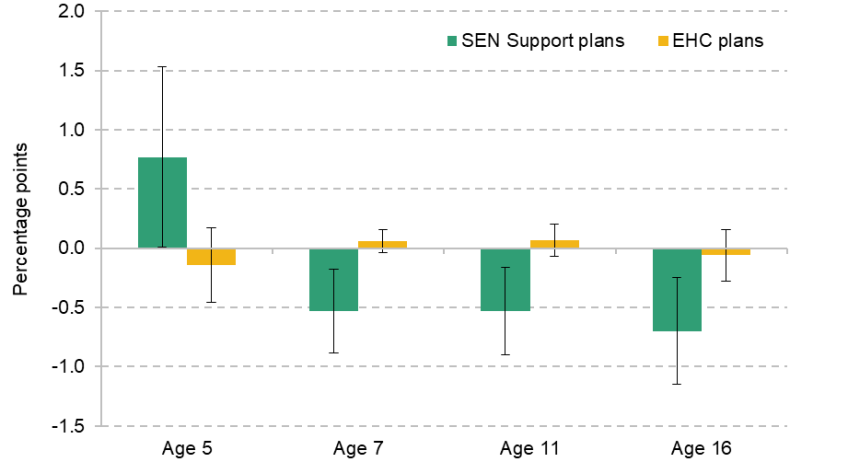
Note: At each age, results represent the difference in the percentage of children receiving support for special educational needs as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
From ages 7 to 16, the story is very different. Children who had access to Sure Start in their early years were 0.5 percentage points less likely to have a SEN Support plan in place at age 7 and age 11, and 0.7 percentage points less likely at age 16. Sure Start therefore reduced the proportion of children receiving support in the medium term, after increasing it in the short run, likely through increased identification of need. Importantly, these medium-term declines in SEN Support plans were concentrated among girls, while the short-run increase was strongest in boys. This means that it is unlikely that the reduction in the medium term was directly attributable to the early detection of additional need, but instead that the improvements in detection and the later reduction in need were two separate effects of Sure Start. Instead, the mechanism behind later effects may have been tailored support for children with high needs at Sure Start centres reducing their need for support in the medium term.
We do not see any evidence that these effects on less severe SEN Support plans extended to effects on more severe EHC plans. At each age, the effect of Sure Start on the proportion of children with EHC plans was not statistically significant.12 This suggests that light-touch early years services, on their own, are not enough to prevent or reduce the impact of the more serious conditions that tend to warrant EHC plans.
6. Effects on hospitalisations and health
6.1 Any-cause hospitalisations
Figure 6.1 reports the estimates of the effect of increased access to Sure Start on the probability of any hospitalisation at each age in the neighbourhood–quarter-of-birth–gender ‘cell’. To account for the fact that the probability of any hospitalisation is very different at different ages, we rescale the effects we estimate by the baseline probability of a neighbourhood having any hospital admission to obtain effect sizes that can be consistently interpreted across ages. These effect sizes therefore give the percentage change in hospitalisation probability, as compared with the baseline probability.
Figure 6.1. Effect of Sure Start on the probability of hospitalisation by age
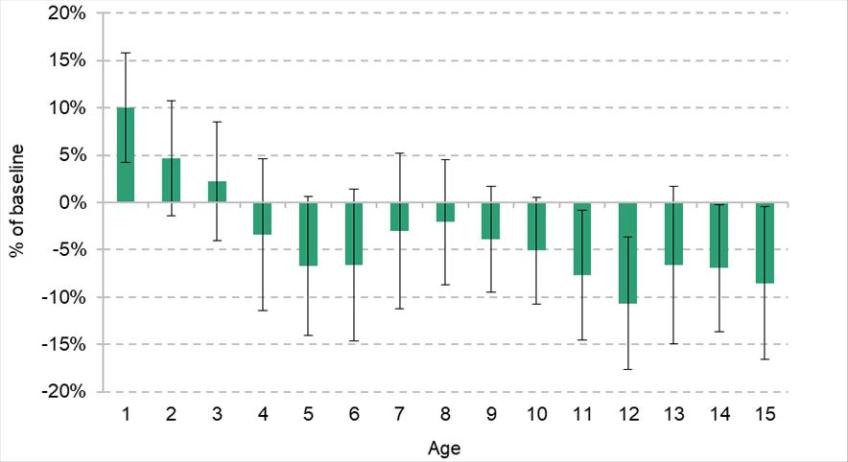
Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
The graph shows that, during the earliest years of life, when children were of an age to use Sure Start services, an increase in access to Sure Start led to an increase in hospital admissions. In particular, an increase of one Sure Start centre per 1,000 children in the local authority raised the probability of any hospitalisation at age 1 in a neighbourhood by 10% relative to pre-Sure-Start levels. That is equivalent to an additional 6,700 hospitalisations per year. Greater access to Sure Start continued to increase hospitalisation at ages 2 and 3, but these effects are smaller and no longer statistically significant.
As children continued to age, these early increases in hospitalisations were followed by substantial decreases in the probability of admission through childhood and early adolescence. Once children turned 5 and stopped being age-eligible to use Sure Start services, the overall impact on hospitalisations became consistently negative, with larger impacts during the first few years of schooling (ages 5–6) and then from age 10 onwards. Increasing Sure Start coverage in the local authority by one centre per 1,000 children at ages 0–4 would have averted around 7% of hospital admissions at age 5 (corresponding to around 2,860 averted hospitalisations a year, though the effects here are not statistically significant). Among 11- and 12-year-olds, an extra centre per 1,000 children averted close to 5,500 hospitalisations a year.
6.2 Cause-specific hospitalisations
As Chapter 3 highlighted, Sure Start could influence hospitalisations through a number of different channels. To disentangle these, we now turn to examining hospitalisations for specific causes (based on the primary condition diagnosed at time of hospitalisation).
Figure 6.2 presents the impact of Sure Start on hospitalisations for ambulatory care-sensitive (ACS) conditions. These include chronic conditions that can typically be managed outside of hospital (e.g. asthma), acute conditions where serious illness could have been prevented by early intervention (e.g. gangrene) and conditions that arise from vaccine-preventable diseases (e.g. measles).
Figure 6.2. Effect of Sure Start on the probability of hospitalisation for preventable causes by age
Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
The graph shows that access to Sure Start substantially increased hospitalisations for these conditions at younger ages, with a 20% increase over baseline levels at age 1. However, as children age, greater access to Sure Start instead reduced ACS admissions, with a 21% reduction over baseline levels by age 11. This could be consistent with greater information, advice and screening in the early years signposting children to healthcare services, which in turn help their families to better manage (or prevent) these conditions in the medium term.
Figure 6.3 shows the effect of increased access to Sure Start on hospitalisations related to infectious or parasitic illnesses. Greater access to Sure Start substantially increased hospitalisations for infectious illnesses in infancy; however, there are significant and substantial falls in hospitalisations (of up to 27% of the baseline) shortly after children ‘age out’ of Sure Start eligibility and start school.
Figure 6.3. Effect of Sure Start on the probability of hospitalisation for infectious diseases by age
Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
This is consistent with exposure to pathogens through Sure Start activities such as childcare, stay and play, or other group-based activities: children who are more exposed early in life are initially more vulnerable to infectious illness, but then build up a stronger immune response which protects them compared with their less exposed peers when the entire cohort enters school. After a few years of schooling, however, these advantages seem to fade out as the immune systems of children with less exposure to Sure Start ‘catch up’ to their peers.
The specific causes of hospitalisations can also shed light on other mechanisms driving different effects of Sure Start. One example of this is the effect on hospitalisations for external causes. These hospitalisations, which include injuries and poisonings, can be loosely defined as hospitalisations not related to illness or disease. They are particularly relevant to our analysis, since there are a number of ways in which Sure Start could affect these outcomes. First, Sure Start provided parents with information on how to make their home safer for young children; this could have reduced both accidents (such as falling down ungated stairs) and poisonings (e.g. from cleaning products not stored safely). Second, Sure Start may have reduced the incidence of maltreatment, either by providing parents with early intervention and support, or by increasing detection rates and helping to remove children from unsafe homes.
Finally, to the extent that Sure Start improved children’s cognitive and socio-emotional development, it could have had longer-lasting impacts on accidents and injuries. For example, a reduction in externalising behaviour could see children behaving in less aggressive or less hyperactive ways. This would plausibly lead to effects growing in the medium term, since older children generally have more freedom for potentially dangerous behaviour that could lead to accidents or injuries.
Figure 6.4 shows that Sure Start led to large declines in hospitalisations for external causes at almost all ages we consider. Unlike the infectious outcomes discussed above, these effects are always negative; even at the youngest ages, the probability of an externally caused hospitalisation fell by 10% or more with greater access to Sure Start. This significant reduction at young ages provides potential evidence for effectiveness through the information channels provided to parents, potentially generating improvements in the safety of the home environment. The continuation of these effects beyond age 5 suggests that these effects on parenting may persist beyond the ages at which families actually use Sure Start, with benefits into the medium term.
Figure 6.4. Effect of Sure Start on the probability of hospitalisation for external causes by age
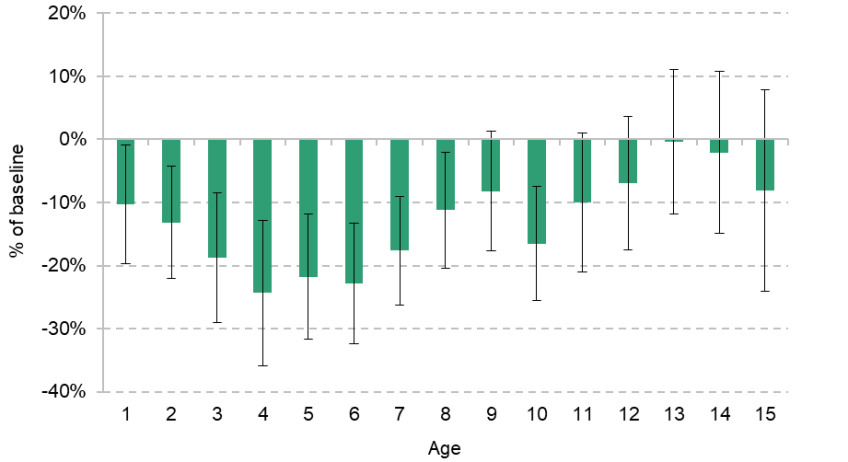
Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
Finally, we report the effect of exposure to Sure Start on children’s mental health.13 There are significant limitations to our data: we only observe hospital admissions, so our measure of mental health is very extreme and does not capture young people who are receiving services in the community, through their schools or through non-hospital providers. Recorded mental health hospitalisations are very rare, and medical guidance typically suggests avoiding mental-health-related diagnoses among primary-school-aged children. We therefore focus on outcomes from age 12 onwards.
Figure 6.5 shows the impact of additional access to Sure Start on mental health admissions among adolescents aged 12–15. We find a statistically significant decrease in admissions related to mental health at ages 12–14. While hospitalisations are a fairly extreme outcome, in Box 6.1 we also present evidence that adolescents who had more exposure to Sure Start earlier in life enjoyed better mental health between ages 11 and 15.
Figure 6.5. Effect of Sure Start on the probability of hospitalisation for mental health causes by age
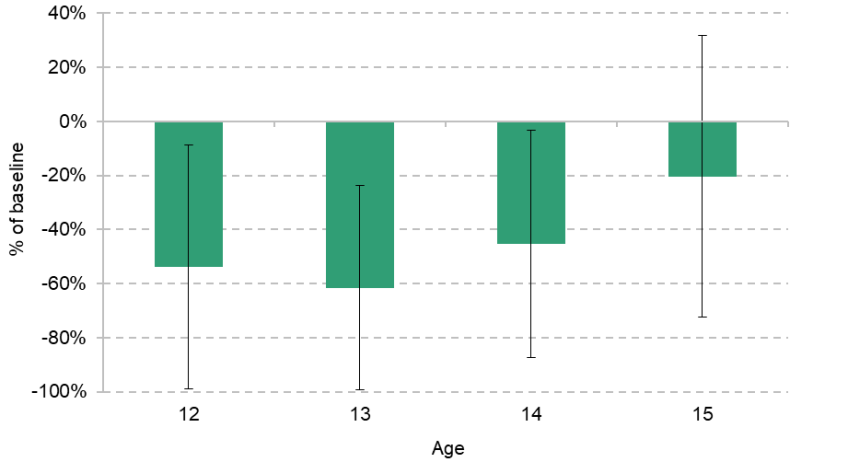
Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
Box 6.1. Results on self-reported health in adolescents
Our main results on physical and mental health are drawn from administrative data on hospitalisations. These data have several advantages, including a large sample size and precise information about the hospital admissions of all children and young people in the sample. However, one downside of focusing on hospital admissions is that we cannot disentangle the impact of a genuine improvement in underlying health from the impact of a change in how people use healthcare.
To shed light on this question, in Cattan et al. (2025) we use an alternative data source: the UK Household Longitudinal Study (UKHLS). The UKHLS (and its predecessor, the British Household Panel Study) is a representative household survey that follows the same group of families each year. It asks young people aged 11–15 about their self-reported physical and mental health.
Because UKHLS is a survey dataset, we cannot implement the same empirical strategy that we use with the administrative hospitalisation records: the sample is not large enough to estimate over 34,000 LSOA fixed effects. Instead, we adopt a different empirical strategy, comparing siblings with more or less exposure to Sure Start. By controlling for family fixed effects, we hold constant many of the features of a young person’s home environment that might influence both access to Sure Start and self-reported health in adolescence.
Table 6.1. Effect of an increase in Sure Start coverage on young people’s self-reported physical and mental health
| V. good or excellent health | SDQ: | SDQ: internalising | SDQ: externalising |
Sure Start coverage | 0.182** | –3.474*** | –2.502*** | –0.960 |
N | 8,047 | 8,192 | 8,197 | 8,195 |
N children | 3,974 | 4,667 | 4,670 | 4,667 |
N families | 1,761 | 2,066 | 2,067 | 2,066 |
Baseline mean | 0.522 | 11.225 | 4.544 | 6.669 |
Baseline SD | 0.501 | 5.443 | 3.031 | 3.659 |
Note: Each specification includes family fixed effects as well as indicators for the year–quarter of birth, the quarter of interview, the age at interview, ethnicity, birth order and whether the household contains any other children aged 0–5, 6–10, 11–15, 16–19 or 20+. Standard errors (shown in parentheses) are clustered at the local authority level. *, ** and *** indicate significance at the 10%, 5% and 1% level, respectively.
Source: Table 4 of Cattan et al. (2025).
We evaluate the impacts of greater access to Sure Start on two different outcomes: overall health (measured by the young person self-reporting ‘very good’ or ‘excellent’ health) and mental health (as measured by the Strengths and Difficulties Questionnaire (SDQ), which assigns higher scores to those with worse social and emotional difficulties). We break down the SDQ results into ‘internalising’ difficulties (e.g. problems with peer relationships or emotional difficulties) and ‘externalising’ challenges (conduct problems and hyperactivity).
We find that young people who had greater access to Sure Start than their older siblings were 18 percentage points more likely to report being in ‘very good’ or ‘excellent’ health. They also reported substantially better mental health, as measured by fewer emotional and behavioural difficulties. In particular, early access to Sure Start seemed to reduce ‘internalising’ behaviours such as emotional difficulties. Compared with the baseline mean, young people with greater access to Sure Start scored around 55% lower on a scale of internalising difficulties than their siblings who had less exposure to Sure Start. Taken together, these results strongly suggest that Sure Start influenced not just the probability of seeking healthcare, but also underlying health (both physical and mental).
Of course, better mental health is a meaningful outcome in its own right. It could also be a channel through which Sure Start affected other long-term outcomes: improved mental health could lead to improved educational performance, reduced need for support with special educational needs, and reduced serious youth offending.
6.3 Authorised absences from school
Another measure of how Sure Start impacted the health of children and young people can be found in school absences. Authorised absences from school – those that are approved by the school as being for a valid reason – are overwhelmingly related to illness.
We therefore explore the impact that access to Sure Start had on authorised absences as a measure of children and young people’s health. In Figure 6.6, we show that school absences among 6-year-olds who had been exposed to Sure Start were around 0.2 percentage points lower than for their peers – equivalent to around a third of a day less absence over the course of the academic year. These results became smaller over time, and were no longer statistically significant by the end of primary school.
Figure 6.6. Effect of Sure Start on authorised school absences by age
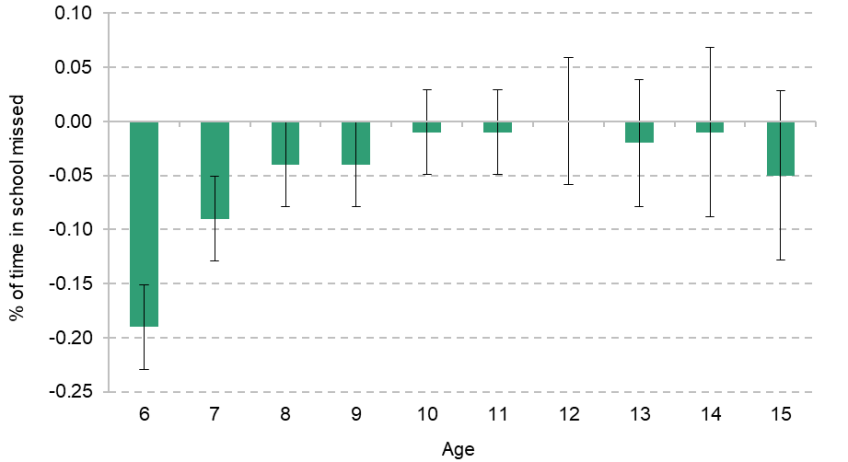
Note: At each age, results represent the difference in the percentage of school days missed for authorised absences as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details. Age 16 is omitted due to the confounding effects of study leave for GCSEs in the summer term.
Source: Authors’ calculations using data from the National Pupil Database.
This is consistent with the results in Figure 6.3, which show that hospitalisations related to infectious illnesses fell sharply at ages 5–6 for children who had been exposed to Sure Start. Effects disappeared later on, as the immune systems of their peers ‘caught up’ after a couple of years in school.
7. Effects on behaviour
7.1 Youth offending
In this section, we focus on the effect of Sure Start on criminal behaviour, which we study by estimating the effect of access to Sure Start on interactions with the youth justice system. Figure 7.1 reports the effect of exposure to Sure Start on criminal offending, broken down by severity of offence. Results are reported as a percentage of baseline levels of each outcome. Overall, the results show that Sure Start generated a statistically significant increase of around 8% in the number of young people with any criminal record by the age of 16. If this increase were replicated nationwide, it would be equivalent to an additional 4,900 young people with any criminal history by the age of 16.
Figure 7.1. Effect of Sure Start on criminal behaviour up to age 16
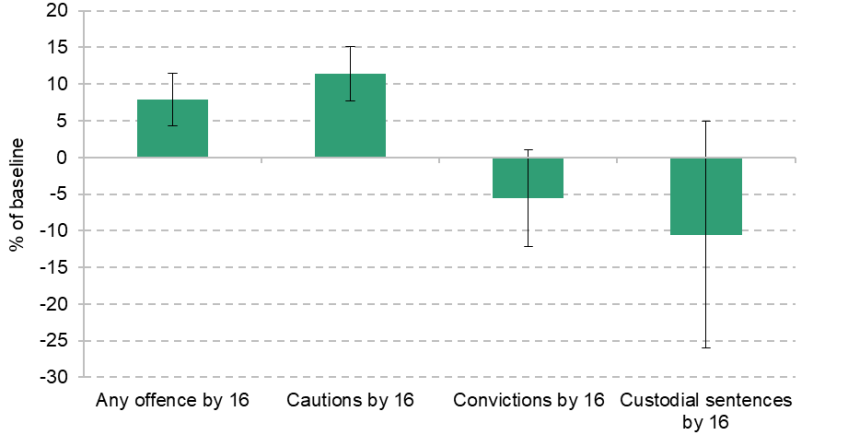
Note: Results represent the effect on the probability of having any criminal offences of the specified type as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
This increase is driven entirely by an increase in the number of young people receiving a youth caution by age 16. The number of 16-year-olds who had received a caution by that age increased by 11% for those who lived near a Sure Start centre – equivalent at a nationwide level to an increase of 6,400 young people receiving a youth caution.14
These negative effects do not extend to more serious criminal behaviour, where we see statistically insignificant drops in interactions with the criminal justice system. Access to Sure Start in the early years led to a 6% drop in the number of young people with a conviction by age 16, and a 11% drop in the number of young people with a custodial sentence by age 16. The lack of significance can be attributed to a lack of statistical power due to the rarity of each outcome, as the effect sizes for both outcomes – and particularly custodial sentences – would represent a major improvement if they represented the true effect of Sure Start.15
Taken together, these results suggest that Sure Start may have reduced the average severity of criminal behaviour for young people, whilst also generating an increase in the frequency of low-level criminal behaviour.16
Figure 7.2 breaks down these results across the five most common categories of offence: theft, drug offences, weapons offences, violent crime and criminal damage, which collectively make up around half of all offences. The graph shows that the increase in cautions is spread across theft, violence and criminal damage. Cautions in these offence categories are typically given out for less severe offences, such as fighting or graffiti.
Figure 7.2. Effect of Sure Start on criminal behaviour up to age 16 by offence type
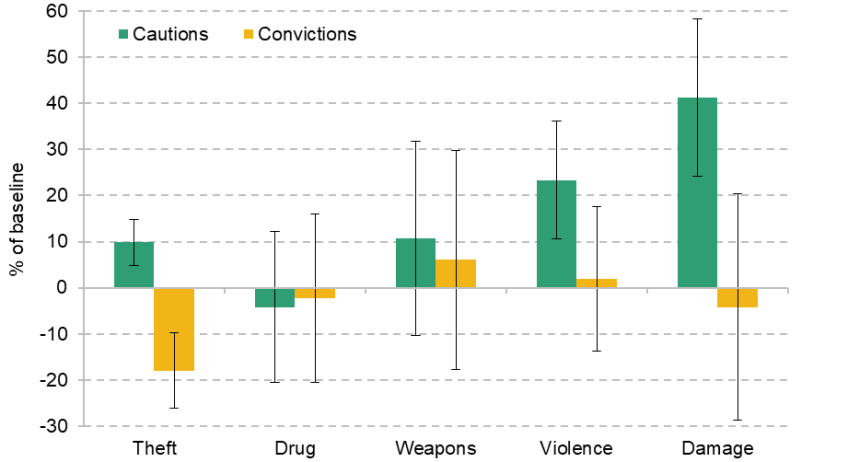
Note: Results represent the effect on the probability of having any criminal offences of the specified type as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
Meanwhile, we do see a statistically significant drop in convictions for theft, the most common cause of convictions. The 18% decline in the number of young people with a theft conviction by age 16 is equivalent to a nationwide reduction of around 1,900, a sizeable drop. It appears this may have marked a shift in severity, as there was a significant increase in the number of young people with cautions for theft, suggesting that those who would have committed more serious thefts shifted to less serious offences as a result of Sure Start.
Figure 7.3 breaks down the effect on cautions and convictions by age, and shows that the increase in cautions is heavily concentrated among younger adolescents. From ages 10 to 12, Sure Start generated statistically significant increases in cautions of over 15%, while the increases in later years were smaller.
Figure 7.3. Effect of Sure Start on criminal behaviour by age
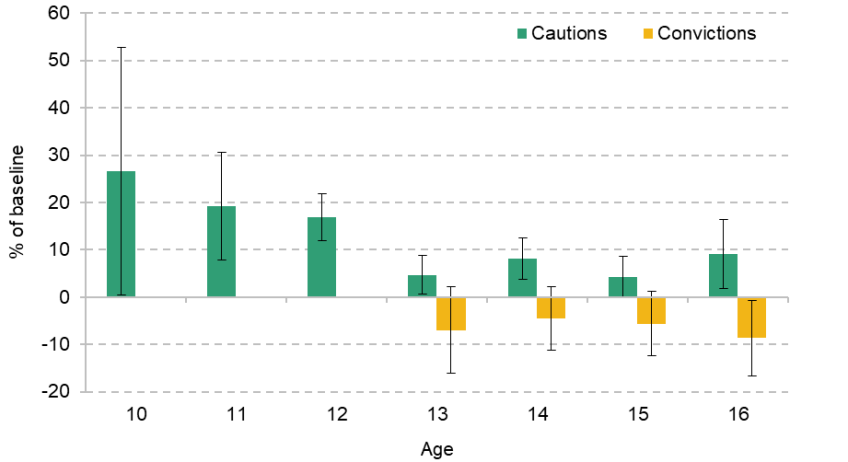
Note: Results represent the effect on the probability of having any criminal offences of the specified type at the specified age as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals, and are removed for the effect of convictions at ages 10–12, where the effect is 0 but convictions are very rare. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
Taken together, Figures 7.2 and 7.3 suggest that the increase in cautions was driven predominantly by younger adolescents committing offences such as fighting and graffiti.
7.2 Unauthorised absences and school exclusions
Further estimates of the effect of Sure Start on behaviour derive from the effect of Sure Start on unauthorised absences from school and exclusions. Figure 7.4 shows the effect of Sure Start on unauthorised absences at ages 6–15. We see statistically significant falls in unauthorised absences at all ages. In primary school, this provides suggestive evidence of changed parenting practices, building on other evidence from the decline in hospitalisations for external causes, as children miss fewer days of school without their school’s permission. In notable contrast to the effect on youth cautions, Sure Start prompted large reductions in unauthorised absences at ages 13–15 – equivalent to around 0.2 fewer unauthorised days missed per pupil per year – which suggest that the significant increases we see in misbehaviour in criminal justice settings did not extend to school settings in the same way.
Figure 7.4. Effect of Sure Start on unauthorised school absences by age
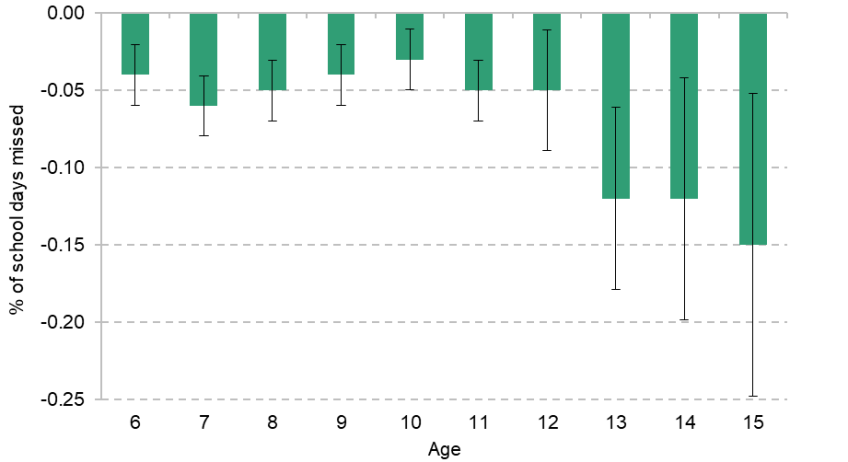
Note: At each age, results represent the difference in the percentage of school days missed for unauthorised absences as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details. Age 16 is omitted due to the confounding effects of study leave for GCSEs in the summer term.
Source: Authors’ calculations using data from the National Pupil Database.
To test effects on misbehaviour in school in another way, we consider the effects of Sure Start on school exclusions in adolescence. We consider both temporary exclusions (suspensions) and permanent exclusions, though approximately 98% of all exclusions are temporary, so the effects predominantly reflect changes in suspensions. Figure 7.5 shows that, as with unauthorised absences, there were particularly large falls in exclusions for teenagers.17 This again suggests that behaviour did not worsen in the way that misbehaviour leading to youth cautions did. However, the age patterns are similar in both outcomes: for unauthorised absences, exclusions and youth cautions, we see evidence of improvements in behaviour at ages 13–16 relative to ages 10–12 (though from different baselines), suggesting that they may reflect similar mechanisms, but with different elements of Sure Start generating different effects for each outcome.
Figure 7.5. Effect of Sure Start on school exclusions by age
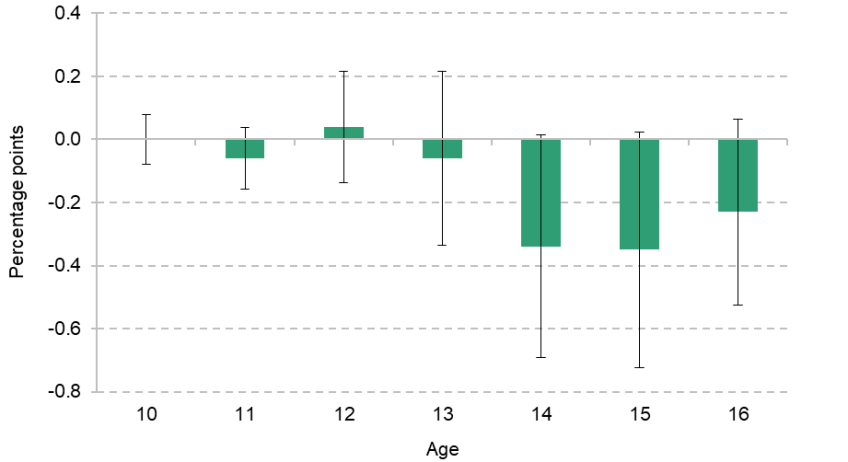
Note: At each age, results represent the difference in the percentage of students receiving a temporary or permanent exclusion from school as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
These reductions in unauthorised absences and exclusions from school may also provide additional explanation for the improvements in academic attainment. More time in school, and less of that time spent causing disruption, may have led to improved educational performance and better test scores.
8. Effects on interactions with children’s social care
This chapter focuses on the impacts of access to a Sure Start centre on school-age children’s contacts with the social care system. Figure 8.1 shows the effect of access to Sure Start on the likelihood of different types of interactions at ages 7–11 with the social care system: probabilities of any referral to social services, any episode of being a Child in Need (CIN) and any period as a Child Looked After (CLA). These experiences range from one of the lighter-touch interactions within the social care system (a referral) to the most intensive (removal into care). We find no significant impact of Sure Start on the probability of these social care contacts (the extensive margin).
Figure 8.1. Effect of Sure Start on interactions with social care, ages 7–11
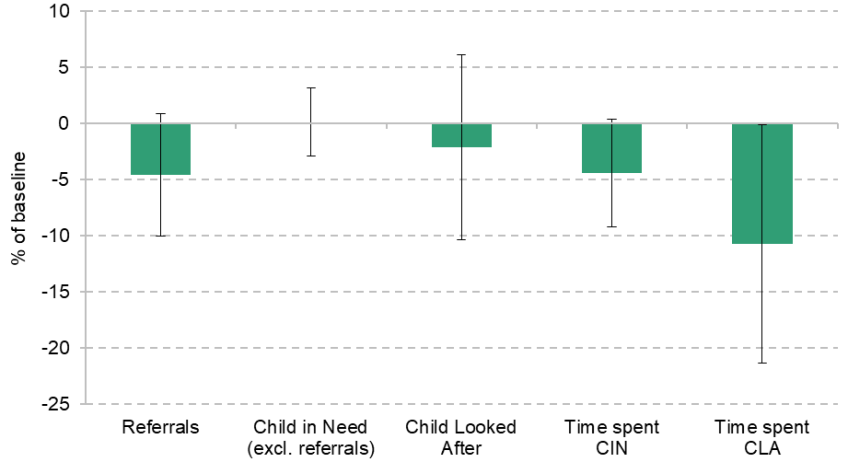
Note: Results represent the effect on the probability of or time spent in different types of interaction with social care services as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National Pupil Database.
The final two points in Figure 8.1 depict impacts of Sure Start on two proxies of the intensity of social care intervention: total time spent as a CIN and total time spent as a CLA between ages 7 and 11. While there is no impact on the time spent as a CIN, there is a sizeable, statistically significant reduction in the time spent in care between ages 7 and 11 of 11%. This suggests that Sure Start may have had some effects on social care, but only by affecting the intensity of need, not the level of need. Therefore, while there is evidence from other outcomes that Sure Start may have affected parenting choices and the nature of the home environment, it does not appear to have generated major effects on more extreme negative outcomes associated with maltreatment or unsafe home environments, though it may have had some effect in the amount of care needed by those in care (the intensive margin).
Figure 8.2 provides further insights into changes in interactions with the social care system by breaking down the effect of Sure Start on different reasons for entering the social care system at the CIN level. There is evidence of a significant drop in the number of children in need due to family dysfunction, suggesting any effects of Sure Start on parenting may have fed through to reduced family dysfunction.
Figure 8.2. Effect of Sure Start on CIN by reason for need, ages 7–11
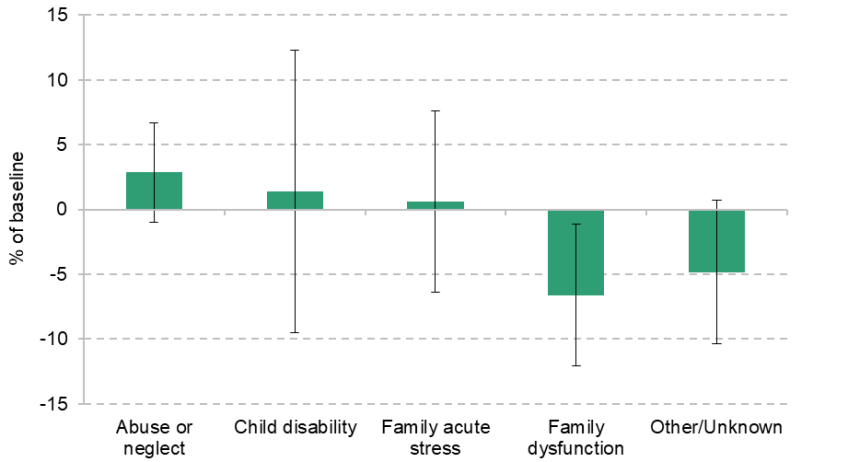
Note: Results represent the effect on the probability of different types of interaction with social care services as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National Pupil Database.
Figures 8.3 and 8.4 show the same results for young people aged 12–15. Unlike at ages 7–11, there is no evidence to suggest Sure Start caused any reduction in interactions with social care on the extensive or intensive margin. In fact, at these ages – where different (earlier) cohorts are analysed due to data availability – there may even have been small increases in the number of children registered as Children in Need due to exposure to Sure Start. This suggests that any improvements to parenting or the home environment that Sure Start might have generated do not appear to have been strong enough to generate reductions in children’s social care at ages 12–15.
Figure 8.3. Effect of Sure Start on interactions with social care, ages 12–15
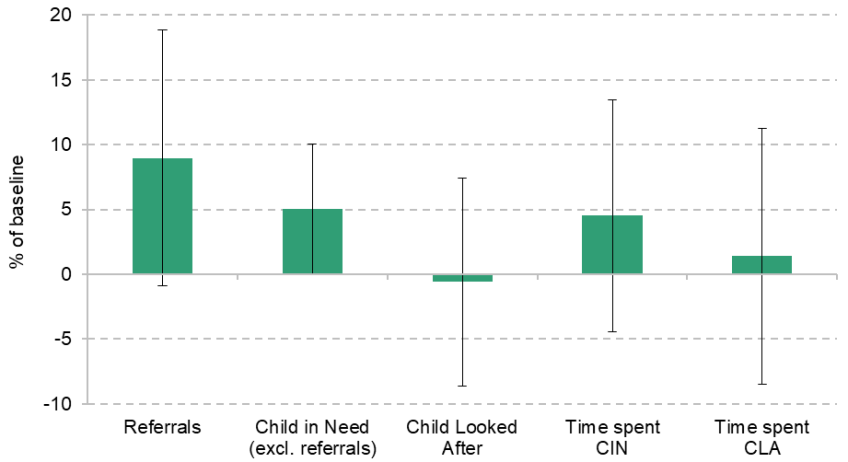
Note: Results represent the effect on the probability of or time spent in different types of interaction with social care services as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National Pupil Database.
Figure 8.4 shows the breakdown of the effect on the number of Children in Need by reason. It shows similar patterns to Figure 8.2, with reductions in the number in need due to family dysfunction, and increases in the number in need due to abuse or neglect, while changes for other reasons are null. While there may be small effects on the margins, this broadly suggests that Sure Start did not have major effects on interactions with children’s social care in the way that it did for other outcomes, and thus that it may not have been a sufficiently intensive programme to generate changes to outcomes as severe as social care usage.
Figure 8.4. Effect of Sure Start on CIN by reason for need, ages 12–15
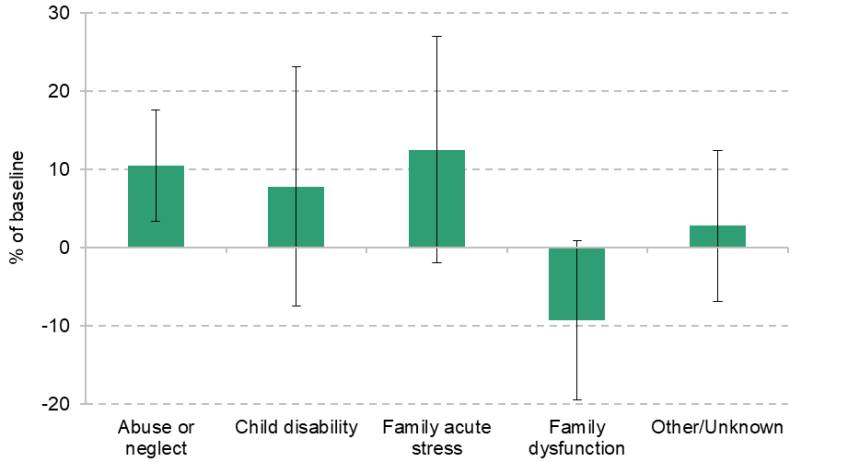
Note: Results represent the effect on the probability of different types of interaction with social care services as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National Pupil Database.
9. Effects of Sure Start by subgroup of the population
In this chapter, we report estimates of the effects of Sure Start for subgroups across three key dimensions of heterogeneity – deprivation, gender and ethnicity – to evaluate whether the effects of Sure Start were evenly spread across the population. We report these effects for several key outcomes to illustrate the relative effects across groups. These are educational attainment, hospitalisation, receipt of SEN Support plans and criminal behaviour.18
9.1 Effects by household income and deprivation
Sure Start was introduced with a specific aim of ameliorating the impact of poverty on children, and the initial roll-out of Sure Start Local Programmes was explicitly targeted to areas with higher levels of local deprivation and areas with high levels of low birthweight and teen pregnancy (Department for Education and Employment, 1999). Over the years we analyse, students from low-income backgrounds had lower academic attainment, higher rates of special educational needs and greater likelihood of having a criminal record by age 16. Therefore, it is important to consider whether Sure Start was as or even more effective for those from low-income backgrounds.
There are reasons to think that Sure Start may have been more effective for these children. Some Sure Start services were particularly relevant to low-income families, such as Jobcentre links, meaning that they could have made more use of the centres. It is also possible that there was more outreach in more deprived areas to encourage families to use services. On the other hand, despite the focus on these services, Sure Start was a universal programme and, by its peak, was available to the majority of the population, including many less deprived areas. It is important to understand whether the decision to expand these services to less deprived families and areas generated significant benefits.
A plausibly significant determinant of the effectiveness of Sure Start for a given child and family is the services and environment that they would have experienced otherwise. Currie (2009) shows that disadvantaged children grow up in less safe and stimulating environments, while Bolt et al. (2021) show that much of the advantage that children from higher-income backgrounds get comes from higher parental investments of both time and money. On the one hand, we might expect Sure Start to partly substitute for deprived home environments for lower-income children, and thus be more effective. On the other hand, it may be that other elements of the home environment in a child’s life might complement Sure Start services, generating larger effects for children who also receive other opportunities (such as if other support or services can help children reinforce things learned at a Sure Start centre).
To study these differences, we run the same analysis presented so far separately for those from low-income households and for the rest of the population. For most outcomes, the indicator of low income we use is eligibility for free school meals (FSM) at age 5, for which 17% of the population we consider qualify.19 Because our analysis of the effects of Sure Start is area-based, these results capture both the effect of using Sure Start and the effect of living near a Sure Start centre on using it. For example, larger effects for FSM-eligible children could be because they got more benefit than other children from using Sure Start or because they were more likely to use Sure Start but got the same benefit from doing so as other children.
Figure 9.1 shows academic results at each age, broken down by whether students are eligible for FSM or not. This shows that with the exception of age 5, where the confidence intervals are very large, the effect of Sure Start for students who were and were not eligible for FSM were similar. At ages 7 and 11, the effect of Sure Start was larger for children from low-income backgrounds, while at age 16 the effects were larger for students from less disadvantaged backgrounds. The difference in effects is only statistically significant for Key Stage 1 tests at age 7.20
Figure 9.1. Effect of Sure Start on attainment by age and free school meals status
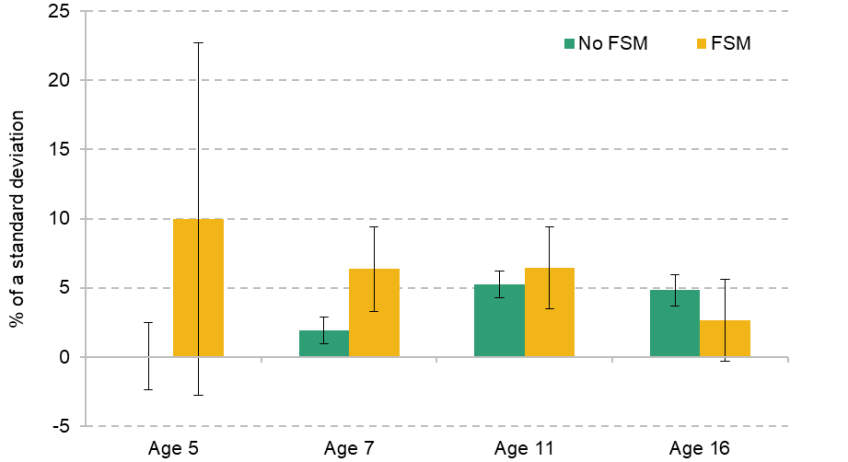
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
For hospitalisations, we do not have access to information on FSM eligibility, so we instead report the effect of Sure Start on the probability of hospitalisation by area deprivation rather than household income. We group areas into three categories based on their ranking on the 2004 Index of Multiple Deprivation: the poorest 30% of neighbourhoods (LSOAs); the richest 30%; and the middle 40%.
Figure 9.2 shows that at age 1, Sure Start only led to an increase in hospitalisations among the 70% most deprived areas of England. For most ages from 9 onwards, Sure Start reduced hospitalisations in the 30% most deprived areas. This suggests that there were larger effects for deprived families, though we do see a drop in hospitalisations for those from wealthier areas at age 5, suggesting that there were some benefits for children in wealthier families. Overall, these results suggest that health services at Sure Start centres may have been relatively more effective for children from more deprived backgrounds than services focused on school readiness were.
Figure 9.2. Effect of Sure Start on the probability of hospitalisation by age and area deprivation

Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
Figures 9.3 and 9.4 show two more key outcomes, the prevalence of SEN Support plans and criminal behaviour respectively, broken down by household income, again proxied by eligibility for free school meals. Sure Start’s role in reducing the need for SEN Support plans in the years after Sure Start attendance does not seem to have varied significantly between more and less disadvantaged households. We only observe a statistically significant increase in SEN Support plans at younger ages for children from less disadvantaged households, but the confidence intervals of the effects on FSM-eligible children are very wide, so we cannot be confident that this reflects greater increases in detection due to Sure Start among children from less deprived backgrounds.
Figure 9.3. Effect of Sure Start on SEN Support plans by age and free school meals status
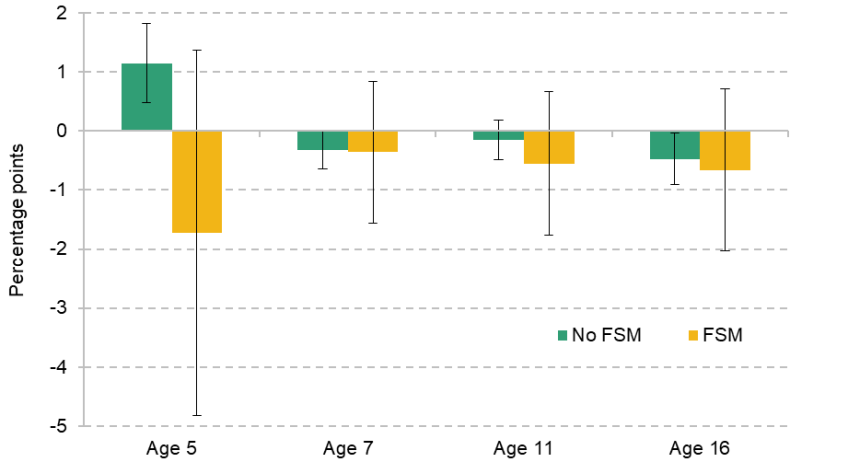
Note: At each age, results represent the difference in the percentage of children with SEN Support plans as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
Figure 9.4. Effect of Sure Start on criminal behaviour up to age 16 by free school meals status
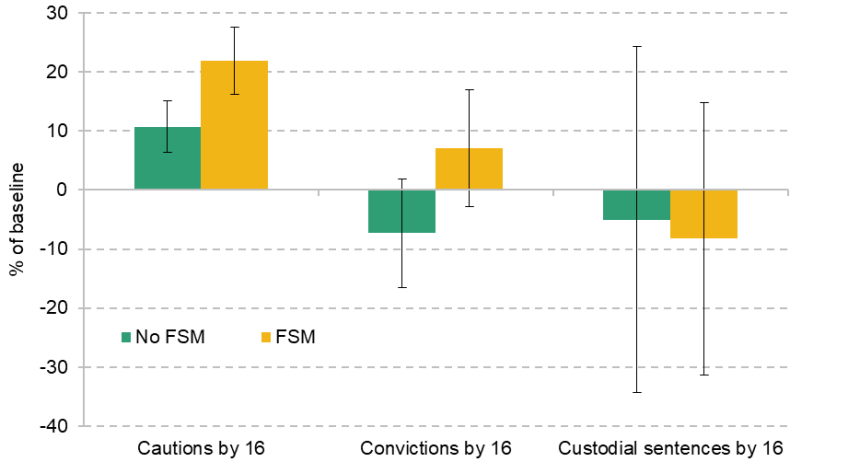
Note: Results represent the effect on the probability of having any criminal offences of the specified type as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
For criminal behaviour, we also see similar effects across all outcomes. The increase in youth cautions is larger for FSM-eligible students, while we see no statistically significant effect on convictions or custodial sentences for either subgroup of students. This aligns with education and SEN results showing no clear pattern of differences in effectiveness across FSM and non-FSM students.
Overall, therefore, it appears that Sure Start had similar effects for families from more and less disadvantaged backgrounds, though there may have been some larger effects for health outcomes. This could be because Sure Start’s services were provided in such a way that they had similar benefits for all users, or because of counterbalancing effects: for example, if Sure Start generated larger academic benefits to children from lower-income backgrounds, but the opening of a local centre was more likely to attract children from less disadvantaged backgrounds, these might generate similar overall effects.
9.2 Effects by gender
Figure 9.5 shows the effects of Sure Start on academic attainment for girls and for boys. The effect sizes are very similar, with no statistically significant differences in effect sizes at ages 5, 7 or 11. However, at age 16, we do see a significantly larger effect for boys. Larger effect sizes for boys would be consistent with the results of evaluations of other early childhood interventions, such as the Abecedarian programme (Conti, Heckman and Pinto, 2016) and Head Start (Carneiro and Ginja, 2014).
Figure 9.5. Effect of Sure Start on attainment by age and gender
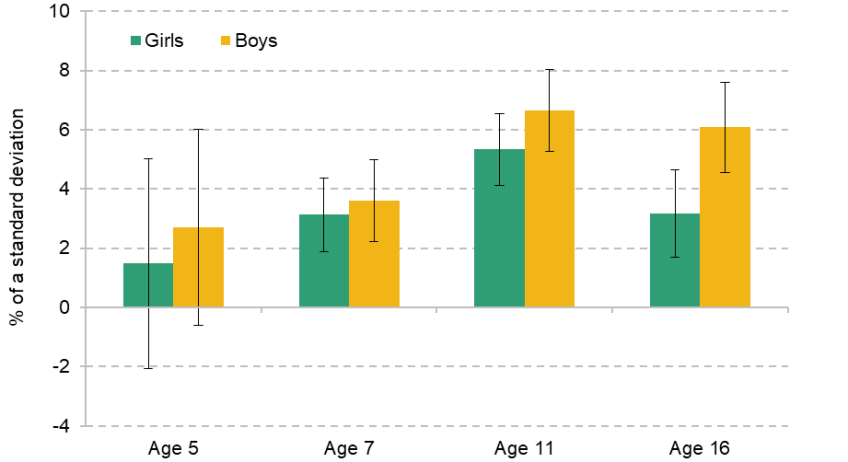
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
Figure 9.6 shows a similar story for hospitalisations, with a similar profile for effects for girls and boys up to age 11, but divergent effects in adolescence. While there is no impact on girls in their teen years, the impact on boys grows steadily, and by age 15 an additional Sure Start centre per 1,000 children during the first five years of life reduces the probability of a hospitalisation by 17%.
Figure 9.6. Effect of Sure Start on the probability of hospitalisation by age and gender
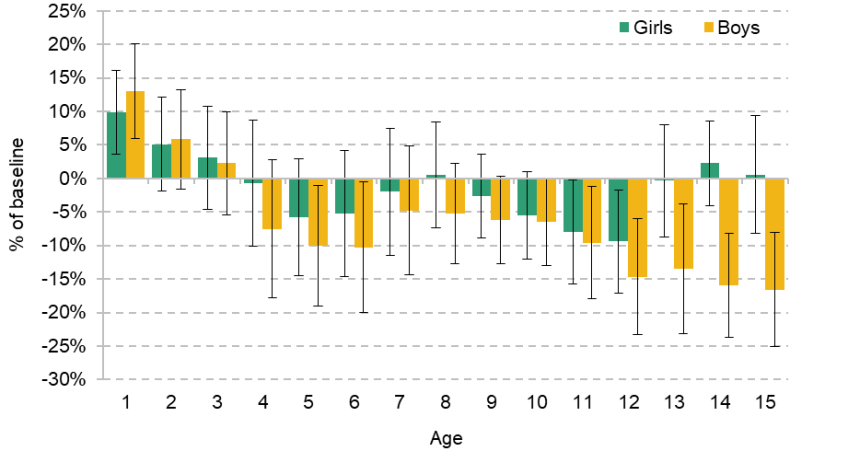
Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
As with educational attainment, the similar trajectories of effects before adolescence suggest these effects are not driven by differences in take-up of Sure Start by gender. For hospitalisations, effects reported in Cattan et al. (2025) show that the gender difference in impacts is entirely driven by a greater impact of Sure Start on reducing hospitalisations for injuries. Injury-related hospitalisations are more likely to happen for boys than for girls throughout childhood, with differences increasing from the age of 11, causing divergent effects from this point onwards.
We see some evidence of gender differences in the effect of Sure Start on the percentage of students on SEN Support plans, as shown in Figure 9.7, though these differences are not statistically significant. Boys appear more likely to be in an SEN Support plan by age 5 as a result of Sure Start, but later in life the reductions in SEN appear to be concentrated more among girls.
Figure 9.7. Effect of Sure Start on SEN Support plans by age and gender
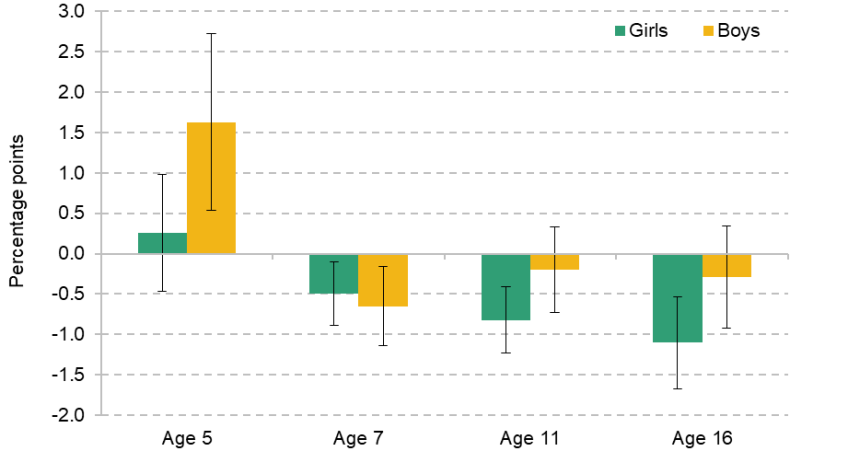
Note: At each age, results represent the difference in the percentage of children with SEN Support plans as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
The disparity in the results for boys and girls suggests, though does not prove conclusively, that the positive overall effect of Sure Start on SEN at age 5 and the negative overall effect of Sure Start on SEN at later ages (seen in Figure 5.3) do not come from the same children: it appears that the positive effect at younger ages was driven by boys, while the negative effect at older ages was driven by girls. This makes it less likely that the story is one of earlier diagnosis leading to a reduction in need in the medium run for the same children.
Figure 9.8 concludes the section on gender differences by showing the differences in effects of Sure Start on youth offending rates. Historically, youth offending rates are much higher for boys than for girls: in our sample prior to the opening of a Sure Start centre, boys are twice as likely to have received a police caution, three times more likely to have received a conviction in court and nine times more likely to have received a custodial sentence by the age of 16. In that context, it is perhaps not surprising that the effect of Sure Start on the total number of convictions and custodial sentences is larger for boys than for girls, as it represents a reduction from a much higher baseline. In percentage terms, however, there are no statistically significant differences in the effect of Sure Start on cautions, convictions or custodial sentences, suggesting Sure Start had similar effects for both boys and girls.
Figure 9.8. Effect of Sure Start on criminal behaviour up to age 16 by gender
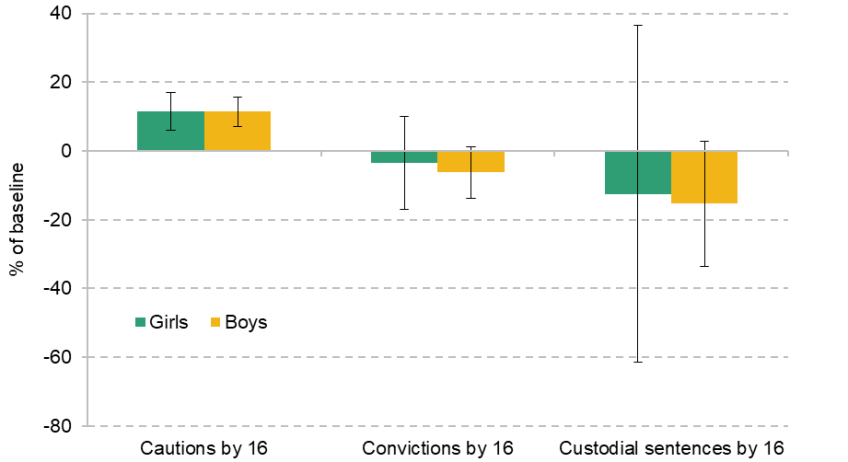
Note: Results represent the effect on the probability of having any criminal offences of the specified type as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
9.3 Effects by ethnicity
Figure 9.9 breaks down the effect of Sure Start on academic outcomes by ethnicity. To ensure our results are precise, we produce estimates of the effects for White students and for students from all non-White backgrounds. These show that at most ages, the effect of Sure Start on grades is much larger for non-White students, though the confidence intervals are still relatively wide due to the smaller number of non-White students.21
Figure 9.9. Effect of Sure Start on attainment by age and ethnicity
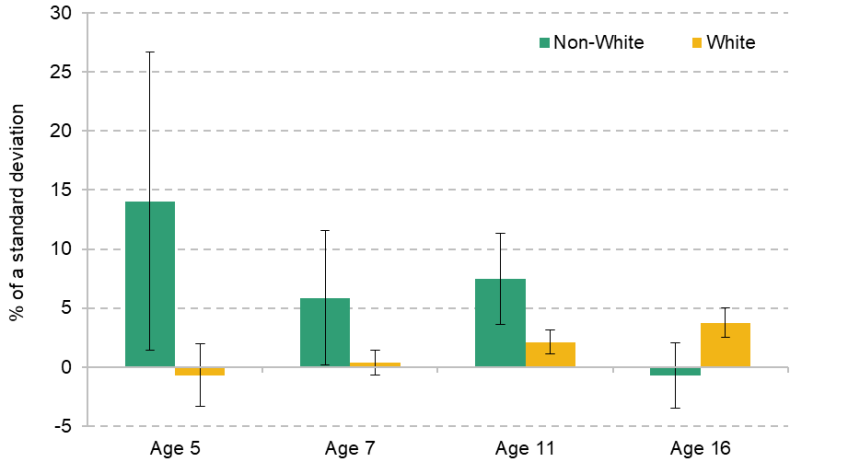
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
Unlike the population as a whole, non-White students experienced a statistically significant improvement in school readiness across all domains as a result of Sure Start, with this improvement continuing on to Key Stage 1 and Key Stage 2 tests at ages 7 and 11 respectively. These larger effects do not appear to have persisted to GCSE results, where we see positive effects mostly driven by White students, but the overall picture appears to be one of larger effects for non-White students. It is worth noting that since non-White children are much more likely to live in urban areas, and we might expect how urban an area is to change the effects of Sure Start, we cannot rule out some of these effects reflecting these urban effects rather than different effects on children of different ethnicities.
Figure 9.10 shows results for SEN Support plans broken down along the same dimensions. We do not see statistically significant differences between White and non-White students at most ages, in large part due to a lack of precision, though there is some suggestion that the drop in SEN Support plans at age 16 may be much larger for non-White students.
Figure 9.10. Effect of Sure Start on SEN Support plans by age and ethnicity
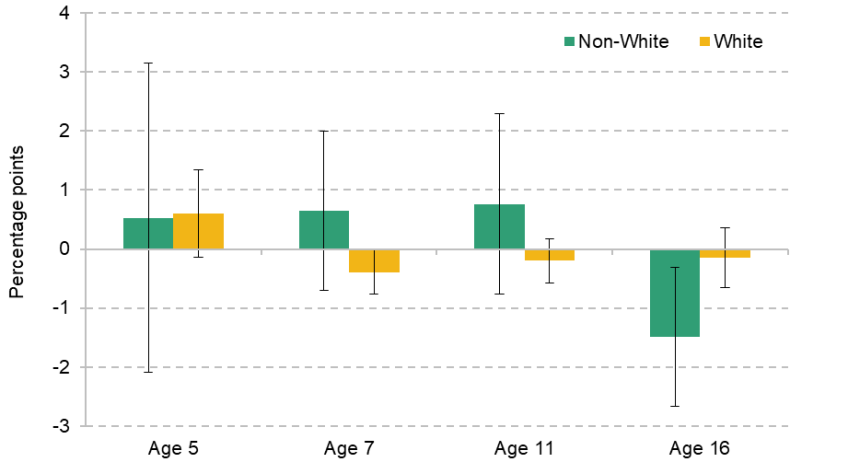
Note: At each age, results represent the difference in the percentage of children with SEN Support plans as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
For criminal behaviour, we see some evidence of larger effects for non-White children, as shown in Figure 9.11. Interestingly, this seems to apply both to larger increases in youth cautions and to larger reductions in serious offending. Non-White young people became 14% more likely to receive a youth caution by the age of 16 as a result of exposure to Sure Start, while White adolescents were not significantly affected. On the other hand, we see a significant drop in the number of non-White children receiving a custodial sentence by the age of 16 – the only subgroup for which we see such an effect. This effect is very large, but with very wide standard errors, due to the rarity of custodial convictions for young people and the smaller number of non-White children in the sample.
Figure 9.11. Effect of Sure Start on criminal behaviour up to age 16 by ethnicity
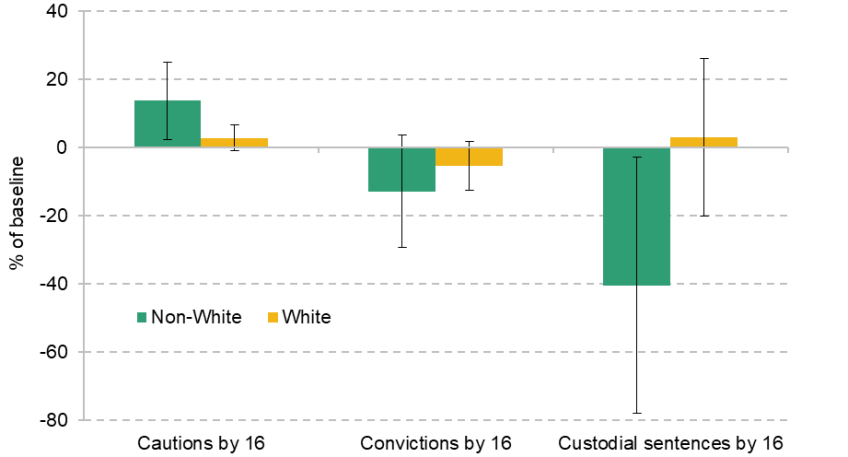
Note: Results represent the effect on the probability of having any criminal offences of the specified type as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
10. Effects of Sure Start by centre context
10.1 Effects by type of neighbourhood
In this section, we analyse the differential effects of Sure Start on urban and rural areas. This provides interesting evidence in its own right, analysing whether Sure Start centres were more effective in urban or rural areas. However, it also serves as a robustness check to ensure that the methods used in this report are sufficient to capture the true effect of Sure Start in two different ways.
First, it is important to understand whether the definition of access to Sure Start as living within 2.5 kilometres of a centre is robust to whether the centre is in an urban or rural area. We might expect families in rural areas to travel further than 2.5km to use a centre, while we might think it would be unlikely that a family living in a very urban area would use a centre 2–2.5km away. Therefore, we use significant effects in both urban and rural areas as evidence that this definition of access to Sure Start is relevant in both types of area (though it is plausible that it is a better measure in one setting than the other, which would make the relative strength of the effects across each type of area harder to compare).
Second, estimates of the effects specifically in urban and rural areas help to show that the results in this report are not driven solely by differential changes across urban and rural areas that happen to be correlated with the opening of Sure Start centres. This might be the case if more Sure Start centres opened in urban areas that happened to improve in certain outcomes around the same time (e.g. if Sure Start centre openings were heavily correlated with the improvement in educational outcomes in London across the 2000s and 2010s). Because we compare treated urban areas with other urban areas as controls, and treated rural areas with other rural areas as controls, significant effects can show that the effects we find in this report are not driven by any decisions to put more Sure Start centres in urban or rural areas.
Figure 10.1 shows the effects on test scores at each age. They broadly show slightly larger effects in urban areas, with a statistically significant difference at age 7. This could reflect differences in the importance of living within 2.5km for use of a centre, larger effects for non-White children, or some other difference between children in urban and rural areas. At ages 11 and 16, we see significant positive effects in both types of area, and at similar levels to the overall effects shown in Figure 5.1. This suggests that the measure of access to Sure Start is relevant in both urban and rural areas and that the effects are not driven by differential changes in outcomes between urban and rural areas that geographical measures of access to Sure Start capture by chance.
Figure 10.1. Effect of Sure Start on attainment by age in urban and rural areas
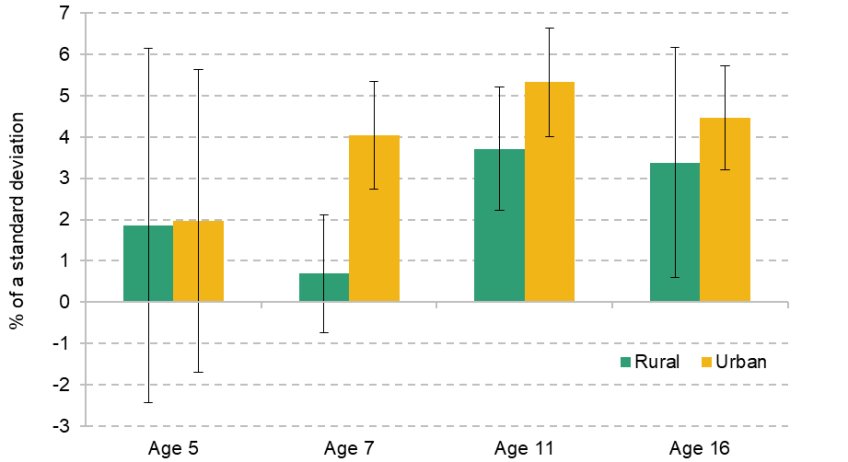
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
We see a similar pattern in Figure 10.2, showing the effect of Sure Start on hospitalisations for both urban and rural areas, with no statistically significant differences in effect sizes at any age, as effect sizes in both types of area track the overall effect, again suggesting that results are not driven by effects in either urban or rural areas.
Figure 10.2. Effect of Sure Start on the probability of hospitalisation by age in urban and rural areas

Note: Results represent the effect of having one additional Sure Start centre per 1,000 children aged 0–4 in a local authority on the probability of hospitalisation in a neighbourhood in that local authority. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from Hospital Episode Statistics.
Figure 10.3 shows the effect of Sure Start on SEN Support plans along the same dimensions. Again we see effects in both urban and rural areas, though we do see some evidence of some effects being limited to one type of area: by age 16, the decrease in the proportion of students with SEN Support plans appears to be limited to children living in urban areas.
Figure 10.3. Effect of Sure Start on SEN Support plans by age in urban and rural areas
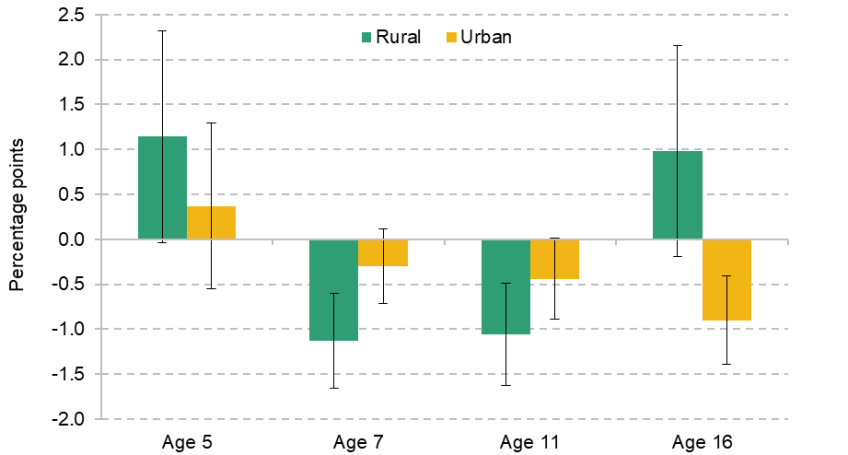
Note: At each age, results represent the difference in the percentage of children with SEN Support plans as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
Finally, Figure 10.4 shows the effect of Sure Start on criminal behaviour for both urban and rural areas. This provides interesting insights into the positive effect of Sure Start on youth cautions, as we see a statistically significant drop in cautions in rural areas and an increase in urban areas. Given that the effects on other types of criminal behaviour and most other outcomes are relatively similar across the two types of area, this suggests that the increase in cautions may be driven by mechanisms unique to urban areas, while in rural areas the improvements in behaviour that can be seen in reductions in unauthorised school absences and school exclusions may have played a bigger role.
Figure 10.4. Effect of Sure Start on criminal behaviour up to age 16 in urban and rural areas
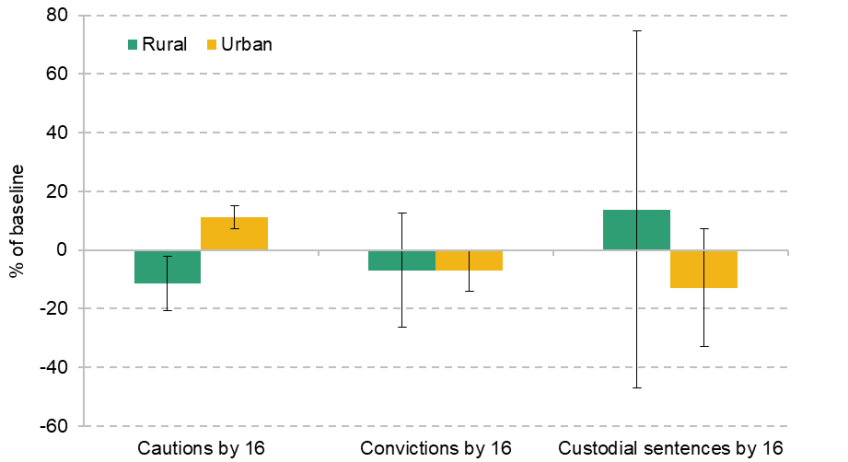
Note: Results represent the effect on the probability of having any criminal offences of the specified type as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National-Pupil-Database–Ministry-of-Justice linked data.
10.2 Effects by type of centre
There are many reasons to believe that the two types of centres – Sure Start Local Programmes (SSLPs) and Sure Start Children’s Centres (SSCCs) – would have different effects on different outcomes. SSLPs had much larger budgets per centre than SSCCs, so we might expect any given SSLP to be more effective than any specific SSCC. This money tended to be spent on extra parental outreach and teacher input into learning development, so if these services were particularly effective we may expect SSLPs to be more effective.
SSLPs also gave local communities a lot more freedom to decide what services they offered, compared with the Core Offer that SSCCs were obliged to provide. While most of the services in the Core Offer were common in SSLPs, the exact structure of the offering was based on a consultation with parents and an assessment of local need. It may be that local tailoring provided additional benefits which boosted the effectiveness of SSLPs, or that the focus of SSCCs on the Core Offer made that relatively more effective.
In order to estimate the differential effects of SSLPs and SSCCs, we consider separately the effect of living near a Sure Start centre that opened up to 2003 and after 2003, when Sure Start Children’s Centres were introduced. This means that we will be including Children’s Centres that were initially Local Programmes as SSLPs. This is still beneficial, as records from the National Audit Office (2006 and 2009) and from Stewart (2013) show that former SSLPs that converted to SSCCs acted quite differently from newer SSCCs, meaning that we are also estimating the effect of this difference in behaviour between the two types of SSCCs.
Figure 10.5 gives the effect of different types of Sure Start centre on academic outcomes at ages 5, 7 and 11.22 Broadly, the effects of the two programmes seem to be similar, and to match the effects of Sure Start overall.23 The possible exception to this is at age 7, where we see about double the improvement in performance for children who grew up near an SSLP compared with those who grew up near an SSCC. However, this difference does not last until age 11, where SSLPs and SSCCs are similarly effective. This could be because the additional budget and offering of SSLPs did not significantly increase effectiveness, or because their effect was counteracted by things making SSCCs more effective, such as focus on the Core Offer or increased choice of centres due to the rapid expansion of the programme.
Figure 10.5. Effect of Sure Start on attainment by age and type of centre
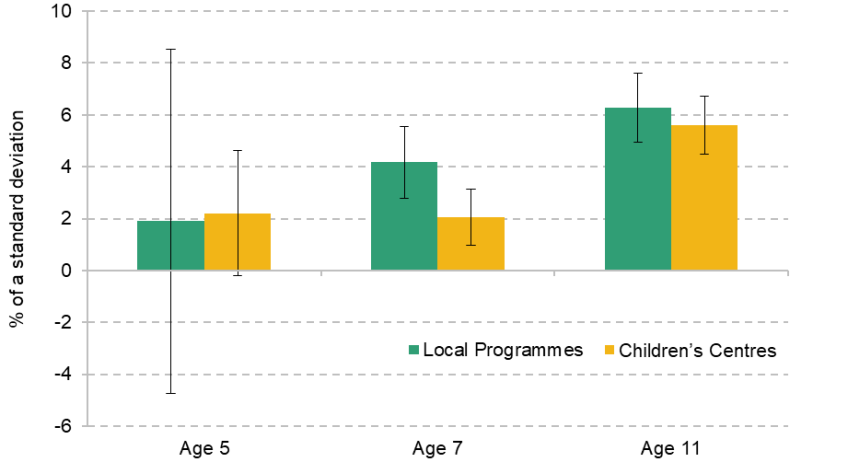
Note: At each age, results represent the difference in test scores as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
Figure 10.6 shows the effects on each type of programme on levels of SEN Support plans at the same ages. As with academic attainment, there is once again no clear pattern in the relative effects of the two programmes. Both appear to generate similar increases in additional SEN Support plans as children stop using Sure Start, before causing a reduction in the percentage of children with plans at ages 7 and 11. SSCCs generated larger reductions at age 7 and SSLPs generated larger reductions at age 11, but the pattern from younger to older ages is similar across both types of centre. This again suggests that both types of centre were effective.
Figure 10.6. Effect of Sure Start on SEN Support plans by age and type of centre
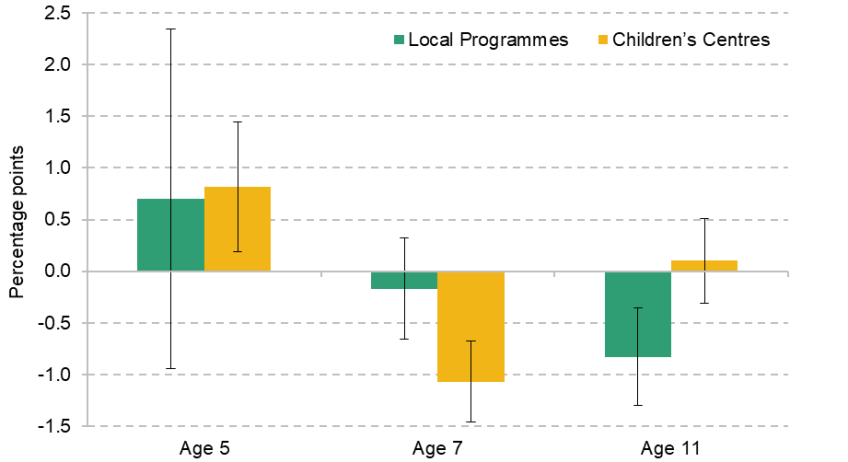
Note: At each age, results represent the difference in the percentage of children with SEN Support plans as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals. The set of cohorts used is different for each age group; see Table 4.1 for details.
Source: Authors’ calculations using data from the National Pupil Database.
We are unable to separate out the relative effects of SSLPs and SSCCs for criminal behaviour, as these estimates derive exclusively from children who lived near SSLPs. We are also unable to draw a distinction in effects for hospitalisation outcomes, due to the different measure of exposure used in this case. For children’s social care interactions, we are able to see effects of both types of centre for secondary-school-aged children, while for primary-school-aged children only the effects of SSCCs are observable.
Figure 10.7 shows the effect of Sure Start on social care interactions between the ages of 12 and 15 for both types of centre. Broadly, the lack of effect from Sure Start extends to both types of centre, with no statistically significant differences in effect size between the two programmes. Across all outcomes considered in this report, there is therefore limited reason to think that one category of Sure Start centre was significantly more effective than the other – though it is not clear whether this is because the differences between them did not play a role in their effectiveness or because they counterbalanced each other.
Figure 10.7. Effect of Sure Start on social care interactions by type of centre, ages 12–15
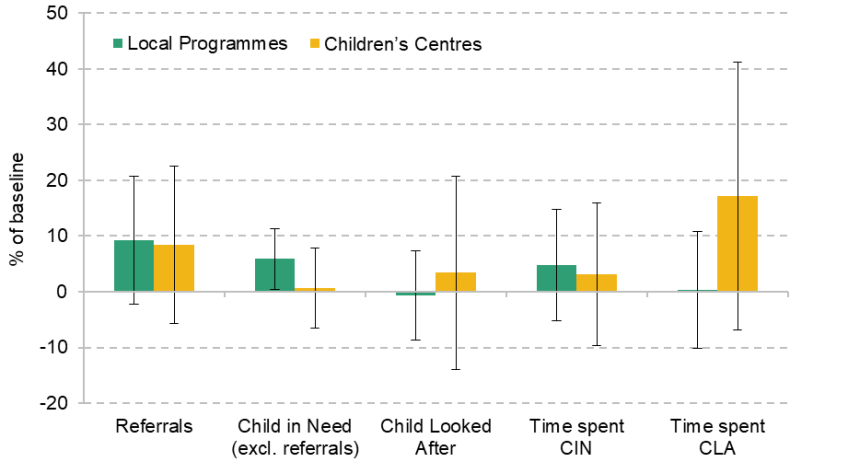
Note: Results represent the effect on the probability of or time spent in different types of interaction with social care services as a result of living within 2.5km of a Sure Start centre, relative to living further away. Error bars represent 95% confidence intervals.
Source: Authors’ calculations using data from the National Pupil Database.
11. Cost–benefit analysis
In this chapter, we draw together the evidence on Sure Start’s impacts on education, health, absences, special educational needs, youth offending and children’s social care. We construct a measure of the financial impacts of all these effects (taking into account the relationships between different outcomes) and compare these benefits with the costs of Sure Start.
We start by rescaling our estimates (which are based on the effect of having access to Sure Start) to estimate the impact Sure Start had on the children who actually used its services. Then, we look at the financial value both to the public purse and to the families and children themselves from the impacts Sure Start had, before comparing the value of these benefits with the costs of the programme.
We focus on the effects of Sure Start across the whole life cycle of the children who attended Sure Start centres. This means that our estimates include both the direct effects of Sure Start that we observe in this report and indirect effects that we expect to develop over time, including those that are spread across the child’s whole life, such as lifetime earnings. For all outcomes, we use a discounted value from when the child ages out of Sure Start eligibility.24
This is a big exercise, and necessarily imprecise. Attaching financial values to the different impacts Sure Start had relies on assumptions about where those benefits were felt, how long they lasted, and how they relate to later outcomes such as employment and earnings. In Section 11.5, we also discuss the limitations of and uncertainties around this cost–benefit analysis.
11.1 Who was affected by Sure Start?
The results in this report focus on the effects of living near a Sure Start centre, rather than actually using a centre. This is an ‘intention to treat’ effect of the Sure Start programme on individual outcomes. For the effects on hospitalisations, this comes from measures of the density of centres in the local area a child lives in when they are hospitalised. For other estimates, it is marked instead by whether a child grew up within 2.5 kilometres of a Sure Start centre. While the use of this marker provides a relatively precise measure of exposure to a Sure Start centre, it requires an estimate of the effect on Sure Start users and the total number of Sure Start users to be scaled up to the overall effect of Sure Start.25
In order to do this, we need an estimate of how much living within 2.5km of a Sure Start centre increases the likelihood that a family uses Sure Start. The best available data come from surveys in 2012 carried out as part of the Evaluation of Children’s Centres in England (ECCE).26 Using these survey data, we estimate that living within 2.5km of a Sure Start centre made children between 30 and 39 percentage points more likely to use Sure Start services than their peers who lived more than 2.5km from a centre.27
We next assume that it is this difference in the likelihood of attending a Sure Start centre that drives the impacts we find of living nearer to Sure Start. That is, we assume that the potential impact of using Sure Start would be similar for children living within 2.5km and those living further away; the differences in outcomes from living closer arise just because these children are more likely to actually use Sure Start services. Based on this assumption, we can say that the results we find are driven by the 30–39% of the population who only attend Sure Start because they live near a centre. Adjusting for this means effects on Sure Start users that are 2.6–3.3 times larger than the effects of living within 2.5km of a centre.28
We also use the ECCE reports to estimate the total usership of Sure Start centres. Using data from ECCE on the number of children registered at an average centre, as well as the proportion of children who had actually used a centre in the last year, we estimate that 55–72% of children aged 0 to 4 – or between 1.7 million and 2.3 million children – were using a Sure Start centre by its peak in 2010.
For the cost–benefit analysis, we combine our central estimate of the effect on users for different outcomes (2.9 times the effect of living near a Sure Start centre) and our central estimate of the proportion of the population who used a centre (64%) with data on the short- and long-run costs and monetary benefits of these outcomes to get the overall costs and benefits of the policy.
11.2 Effects of Sure Start on the exchequer
Sure Start represented a significant up-front cost to the government. By 2010, England spent over £2 billion (in 2023–24 prices) on the running costs of Sure Start Children’s Centres, in addition to another £0.5 billion of capital spending as new centres were opened. This amounted to total spending of £2.7 billion, which represented around 30% of total spending on the early years (Belfield, Farquharson and Sibieta, 2018). Based on our estimates of usership, this translated to spending around £1,350 per Sure Start user per year by the peak of the programme in 2010.
However, Sure Start’s effects on government spending were not limited to the up-front costs, as many of the outcomes discussed in this report drive government spending or revenues.29 In this section, we estimate how the effects of Sure Start are likely to have translated into savings for the exchequer in the long run. A list of the types of spending and revenue considered can be found in Table 11.1 later. All savings are reflective of estimates for the effect on one cohort of children in 2010, compared with the cost of providing Sure Start services to that cohort across all five years of eligibility at the peak of the programme.30
Health
For the costs of the health outcomes of Sure Start, we focus on both the short- and long-run costs to the government from increased hospitalisations. The most direct of these costs is the cost of the hospitalisations we observe in the data themselves. We use cause-specific cost data across injuries, poisoning, respiratory conditions, infections and mental health. In total, the direct savings from reduced hospitalisations at ages 1–15 are less than £10 million per year. Despite hospitalisations being relatively expensive, and the effects being large relative to the baseline, the baseline frequency of hospitalisations is rare enough that the monetary effects are not that large.31
There are larger effects from some of the improvements in health that underlie the reductions in hospitalisations. For example, we found that greater access to Sure Start significantly reduced head injuries (Cattan et al., 2025). These injuries, particularly traumatic brain injuries, can generate significant long-run costs, through both medical expenses and spending on disability benefits. Therefore, we estimate that by reducing the frequency of head injuries, Sure Start is likely to generate a £50 million reduction in lifetime medical spending on those who would otherwise have suffered a traumatic brain injury and a £200 million reduction in lifetime welfare spending on the same individuals (both discounted). In total, these savings from fewer hospitalisations, improvements in health and reductions in severe conditions such as traumatic brain injuries represent just under 10% of the up-front cost of Sure Start.
Special educational needs
Access to Sure Start drove a significant reduction in the number of children with SEN Support plans over the course of their time in school. Data on the costs of this support are taken from the notional SEN budget for mainstream schools. This budget assumes that the average cost for supporting a child with SEN is £3,000. Incorporating the effects of Sure Start throughout childhood, this implies total averted costs of £200 million a year by 2010. We do not consider any savings that may have come from changes to the number of students with Education, Health and Care plans, as we do not observe any statistically significant effects as a result of Sure Start.
Children’s social care
For the effect of Sure Start on spending on children’s social care, we focus on the effect of Sure Start on the total amount of time that individuals spend either as Children in Need or as Children Looked After. We do not find statistically significant effects from Sure Start on the total amount of time spent as a Child in Need, but we do see a significant drop in the amount of time spent as Children Looked After from age 7 to 11. Time spent as a Child Looked After is very expensive: an additional month spent in care for a single child cost around £4,700 (in 2023–24 prices) in the middle of the 2010s. The reductions in time spent in care as a result of Sure Start are therefore enough to generate savings of £110 million.
Youth justice
Youth crime imposes significant financial costs on the justice system, through policing, the courts and offender management programmes. We consider the costs to the court system of each conviction for a young offender, taking account of specific costs for different categories of offence. We also consider the policing costs that come with each caution or conviction, the costs of youth custody, and the offender management costs that are roughly proportionate to the number of young people with any criminal history.
Because we do not see significant effects of Sure Start on most categories of criminal behaviour, we only use two costs in Table 11.1. These are the cost of processing theft convictions in the courts (as these drop significantly as a result of Sure Start) and the cost of offender management programmes (as the total number of young people with any criminal history increased, given a rise in youth cautions). These savings and additional costs are both relatively small, in the order of about £10 million, and they roughly balance out – so we conclude that Sure Start had almost no impact on justice spending.
We do not attempt to estimate the long-run effects of Sure Start on the cost of crime, though evaluations of other similar early years interventions such as Head Start in the US have found significant long-run effects and savings through this channel (Anders et al., 2023). Unfortunately, there is a lack of good evidence in the UK on how a change in criminal behaviour during adolescence shapes later crime. We also note that the increase in cautions that we found was concentrated in younger ages, with much smaller effects by age 16 (the latest age we can study). Given this pattern of fade-out and the very small net financial impact we find during adolescence, we would not expect including the long-term costs of crime to significantly change the picture presented here.
Changes to taxes on income
Aside from the up-front costs of the programme, the most consequential effects of Sure Start to the exchequer are those that come from increased tax revenue. The long-run effects of Sure Start on earnings – the details of the estimates of which can be found in the next section – should also lead to an increase in revenue for the exchequer, due to the increased income tax and (employee and employer) National Insurance contributions paid on increased earnings.
Our rough estimate of the proportion of these increased incomes that would go towards the government is 43%, based on the marginal tax rate of an individual paying the basic rate of income tax and earning between the primary threshold and the upper earnings limit for National Insurance contributions.32 Combining this with estimates of the long-run earnings returns to Sure Start access implies an estimate of a £1.9 billion increase in discounted tax revenue across the attending cohort’s lives as a result of Sure Start.
Of course, the precise number is subject to considerable uncertainty: to arrive at it, we need to model how outcomes in adolescence will translate into earnings over the life cycle. And it will matter to the public purse whether there is a small impact on the earnings of a large number of people, or a large impact on few people (and whether those people would otherwise have been high or low earners). So this estimate of the increase in tax revenues gives a sense of the potential scale, rather than a precise forecast for Sure Start’s impacts on the public purse.
11.3 Benefits to individuals from Sure Start
In addition to averted exchequer costs and increased revenues from Sure Start, several of the outcomes considered in this report are associated with significant private benefits to individuals. These wider benefits will not directly affect the public purse, but they are still valuable and important to capture in a full cost–benefit analysis.
Long-run earnings
The largest individual benefits from Sure Start stem from the expected effect on long-run earnings. To estimate this, we use the effect of the programme on GCSE grades to obtain an estimate of the long-run benefits of the improved educational attainment generated by Sure Start. Hodge, Little and Weldon (2021) estimate that a one standard deviation improvement in GCSE performance translates to a £117,190 increase in discounted lifetime earnings (in 2023–24 prices). Applying these estimates to our findings of an improvement of 4.7% of a standard deviation as a result of exposure to Sure Start gives an estimated increase in lifetime discounted earnings from age 5 of £13,000 from using Sure Start. Of that, a significant proportion goes towards taxes, leading to an increase in lifetime post-tax earnings for the average Sure Start user of about £7,800. Across all users, this adds up to a total increase in discounted post-tax earnings of £3.1 billion, larger than the up-front cost of Sure Start in itself. Again, it is important to stress that this is an estimate based on Sure Start’s impacts on educational qualifications at age 16: using these results to project the impacts on long-run earnings is, by necessity, subject to considerable uncertainty. To avoid double-counting different effects, we do not consider the effect of other outcomes we look at on long-run earnings, since they may overlap with (or contribute to) the effects on earnings that arise via higher educational attainment. For example, while Sure Start reduced absences, it is unlikely that this reduction in absences impacted lifetime earnings over and above the improvement in test scores that we capture directly.
However, this means that we may be missing any effects on earnings that arise through channels other than improved GCSE performance in school. For example, if the effects on outcomes such as criminal behaviour and social care interactions in this report lead to changes in long-run earnings, they would likely not be fully reflected in changes to GCSE results. Of course, these effects could go in either direction, given the presence of both positive and negative effects in these areas.
Health
In addition to averting costs for the NHS and the wider public purse, Sure Start’s impacts on health also generated savings for the children and families who used the centres. Some of this comes from savings for families: since the hospitalisation of a child often leads to lost earnings, there are benefits to family earnings from reducing hospitalisations (though, in practice, the total scale of these earnings benefits is very small).
Other benefits apply to the children, from likely reductions in traumatic brain injuries and child maltreatment reflected in reduced hospitalisations for injuries and external causes. We include the savings to individuals from avoiding traumatic brain injuries, in the form of reduced care costs (savings covered by disability benefits are already reflected in the savings to the exchequer described above). Similarly, we include the benefits of avoiding very rare but costly cases of fatal maltreatment. In combination, the financial benefits to individuals flowing from Sure Start’s impacts on health add up to approximately £20 million by its peak.
Criminal behaviour
In addition to generating costs for the state, most criminal behaviour also generates costs for the victims of crime. We therefore include the effects of changes to criminal behaviour on victims in the effects on private individuals. For this, we consider the effects of both cautions and convictions, taking into account the different categories of crime where we find that Sure Start had a significant effect. We assume that the increase in youth cautions that resulted from greater access to Sure Start perfectly reflects an increase in underlying crime (rather than changes in detection or reporting). We estimate that the victims of crime lost around £40 million in damages per cohort due to the increased prevalence of minor violent offences, thefts and criminal damage incidents.
11.4 Comparing costs and benefits
Table 11.1 provides a summary of all the benefits and costs of Sure Start considered in this report. They are separated into the up-front cost to the government of running and expanding the Sure Start offering; changes in spending and revenue for the state as a result of the effects of the policy; and benefits and costs for private individuals.
Table 11.1. Costs and benefits of Sure Start
Up-front costs | Value |
Up-front cost of Sure Start per cohort | £2,690m |
Savings to the government | Value |
Increased long-run tax revenues | £1,860m |
Reduced short-run hospitalisations | £10m |
Reduced long-run hospitalisations | £50m |
Reduced spending to support people with traumatic brain injury | £200m |
Reduced spending on SEN Support plans | £200m |
Reduced spending on Children Looked After | £110m |
Changes to spending on policing and courts | ~£0 |
Total savings to the government | £2,420m |
Benefits | Value |
Increased long-run post-tax earnings | £3,110m |
Reduced long-run costs of traumatic brain injury | £10m |
Reduced risk of fatal maltreatment | £10m |
Savings to parents from reduced time in hospital | ~£0 |
Increased victimhood from youth crime | –£40m |
Total benefits | £3,090m |
Note: Negative values for benefits reflect monetary losses. Values may not sum due to rounding. Estimates for lifetime benefits are central projections based on best-available estimates in the literature, but are subject to considerable uncertainty.
There are two ways of comparing the benefits and costs of the policy. The first is to compare the sum of all benefits, across both private individuals and the government, with the up-front cost of the policy. By this metric, for every £1 the government spent on Sure Start centres, there were societal benefits of £2.05. This represents a large benefit for the cost, and at a significant scale: the programme generated £2.8 billion more in benefits than its up-front cost.
The second way to compare the benefits and costs of the policy is to draw a distinction between benefits to private individuals and to the government. By our estimates, the total net cost of Sure Start to the government, once all long-run savings are taken into account, was around £270 million: 90% of the up-front costs will eventually be recouped in long-run savings. This means that Sure Start’s benefits to the public purse (eventually) offset much of the initial investment, but that Sure Start did not entirely ‘pay for itself’ from the government’s perspective.
Still, if the net public outlay on Sure Start was less than £300 million, then our central estimate of the private benefits of around £3.1 billion was more than 11 times as large as the programme’s long-run net cost. This represents a very strong return to the investment, and aligns with similarly large returns to integrated early years programmes such as Head Start in the US (Hendren and Sprung-Keyser, 2020). Importantly, this approach to calculating the ‘marginal value of public funds’ is highly sensitive to the estimated long-run savings to government: if the actual impact on earnings and taxes were 10% lower than we estimate here, for example, this marginal value of public funds measure would fall to a ratio of £6.09 return for every £1 of net spending.
11.5 Potential limitations
The cost–benefit analysis in this chapter pulls together evidence on a range of outcomes measured over a long period. As with any cost–benefit analysis, it necessarily relies on many assumptions about how long the benefits will last, which benefits overlap and could be double-counted, how early benefits in terms of education and health relate to later earnings, and how individuals and the public purse value these different benefits. All of this means that the estimates presented here give a good sense of how the scale of benefits compares with the scale of the programme’s costs – but the precise numbers themselves are estimates with considerable uncertainty attached.
There are several ways in which the cost–benefit analysis outlined in this chapter might overestimate or underestimate the monetary benefits or costs associated with Sure Start. The first is through outcomes that are not included in this analysis. These include outcomes past the age of 16 in criminal offending, hospitalisations and social care, as well as effects on children’s social care at ages younger than 7. Healthcare costs from primary care are also omitted, as are effects on earnings that cannot be explained by improved educational attainment. While we might expect Sure Start to have generated more benefits than costs through these channels – leading to an underestimate – the role of increased service use means in some areas this analysis could also generate an overestimate.
The most significant omission from this analysis is the offering of the services themselves.
Most Sure Start services were offered free of charge or at a reduced price. For parents who would have paid for these services, this represents an in-kind transfer that is valuable to the families. But since it is uncommon for integrated services such as those offered at Sure Start centres to be offered privately, it is difficult to estimate families’ willingness to pay for the services that they received for free.
In some cases, families likely have very little willingness to pay. Many Sure Start centres had a significant focus on outreach and persuading families to take up the services offered at Sure Start centres; these families are unlikely to have had a high willingness to pay out of pocket for these services.
It is more likely that families would have been willing to pay for other elements of the Sure Start offering such as play sessions or easier access to children’s healthcare, and so the offering of these services for free should be thought of as an additional benefit. However, it is not possible to disentangle families’ demand for these services from the long-run benefits that they bring to children, and so we are not able to provide a numeric estimate for the value they place on these services beyond the benefits to children and families discussed in Section 11.3.
Outcomes discussed in this report also bring significant non-monetary benefits for which families might be willing to pay, but which are not possible to quantify. For example, improved health is likely to bring benefits to individuals beyond those that are captured in the financial costs for individuals and the government of supporting those with health problems. A similar story may also apply to changes in educational attainment, criminal behaviour and interactions with children’s social care. This chapter excludes any of these non-pecuniary benefits from these outcomes from the analysis.
There are also limitations to the method by which effects of access to Sure Start are scaled into overall effects. It assumes that all attendees of a centre get the same benefit – if users who lived further away got a smaller benefit from the programme (e.g. because they used the services less intensively or they had different characteristics), then this method would overestimate the effect on nearby users. Additionally, data on location and usership are taken from only a sample of centres, rather than capturing the relationship between distance and Sure Start usage across the whole population.
Finally, these results are limited by the fact that the data in ECCE are taken from a survey in 2011 and 2012. As a result, we focus on the effect of Sure Start at its peak (and the last year we study) in 2010, when service usage is likely to have most closely matched usership rates in the ECCE report. However, as our estimates reflect the effects on cohorts born earlier than this, we adopt the underlying assumption that the effects were constant across years. This is supported by the fact that earlier and later centres were similarly effective. If, however, centres had become more or less effective by 2010, then our cost–benefit analysis would represent an underestimate or overestimate respectively of the true returns to the policy at its peak. Furthermore, the ratio of costs to benefits in earlier years should not necessarily be assumed to be the same: earlier centres spent more per child living nearby, which might mean they had lower benefit–cost ratios.
12. Summary and policy implications
In England, Sure Start pioneered the concept of an early years programme that provided a comprehensive range of services under one roof, incorporating health services, parenting support and childcare in the same centre.
As one of the country’s largest early years policies, evaluating the impacts that Sure Start had on children is important in its own right. Bringing together a wide range of outcomes – capturing different dimensions of children’s development and more and less serious outcomes – gives us a unique opportunity to learn about how integrated early years services affected children and young people in the round. And, because the roll-out of Sure Start began more than 25 years ago, an evaluation today also lets us explore the long-term effects that Sure Start had.
While Sure Start itself is much less a feature of the early years landscape than it once was, the lessons it holds for designing and implementing early years services remain just as relevant today as they once were. The new Family Hubs and Start for Life programme, which seeks to bring together a range of family support services, and similar initiatives in the rest of the UK – including Flying Start in Wales and the continued Sure Start programme in Northern Ireland – and internationally can also draw on the lessons learned from this evaluation.
12.1 Summary of results
Table 12.1 provides a summary of the signs and statistical significance of the impacts of Sure Start on the range of outcomes this research has considered.
Table 12.1. Summary of key outcomes
Outcome group | Outcome | Effect direction | Statistically significant? |
Academic attainment | FSP score | ↑ | No |
Key Stage 1 score | ↑ | Yes | |
Key Stage 2 score | ↑ | Yes | |
Key Stage 4 score | ↑ | Yes | |
SEN Support plans | Age 5 | ↑ | Yes |
Ages 7, 11 and 16 | ↓ | Yes | |
Education, Health and Care plans | Age 5 | ↓ | No |
Ages 7, 11 and 16 | ↓ and ↑ | No | |
All-cause hospitalisations | Ages 1–3 | ↑ | At some ages |
Ages 4–15 | ↓ | At some ages | |
Youth offending | Total offences | ↑ | Yes |
Cautions | ↑ | Yes | |
Convictions | ↓ | No | |
Custodial sentences | ↓ | No | |
School-related behaviour | Authorised absences | ↓ | At some ages |
Unauthorised absences | ↓ | At some ages | |
Exclusions | ↓ and ↑ | No | |
Interactions with social care | Child in Need, ages 7–11 | ↑ | No |
Child Looked After, ages 7–11 | ↓ | No | |
Child in Need, ages 12–15 | ↑ | No | |
Child Looked After, ages 12–15 | ↓ | No |
Wide-ranging benefits – but no silver bullet
Overall, our results confirm that Sure Start promoted several dimensions of children’s capabilities. Early access to Sure Start improved test scores; reduced hospitalisations in childhood and adolescence; reduced school absences and exclusions; and reduced the share of children receiving less intensive support for special educational needs. This portfolio of results strongly suggests that early access to Sure Start shaped children’s cognitive, physical and social development as well as their environments and use of services at home and school.
But our results also suggest that light-touch, universal early years services are not a ‘silver bullet’, particularly for avoiding the need for intensive, specialist services. We find no effects on Education, Health and Care plans. While interactions with the children’s social care system tended to fall during primary school among children with access to Sure Start, contact amongst secondary school pupils was often higher (though these results were generally not statistically significant). We also find that children with early access to Sure Start were more likely to receive a caution (though less likely to have a conviction or custodial sentence) by age 16. While integrated early years services can benefit children’s lives in a long-lasting way, it is unrealistic to expect that early years services will ever completely replace the need for later, more specialised interventions.
Long-lasting benefits
Remarkably, across almost all the outcomes we consider, the effects of Sure Start are visible from early childhood all the way through primary school and adolescence. While this result is in line with what we could expect from an early childhood programme that puts strong emphasis on promoting child development, this finding is still remarkable given the large number of early childhood programmes whose effects fade out quickly after the programme ends.
The evidence we gather in this report suggests that several channels may be responsible for the persistence in impacts. First, Sure Start directly shaped children’s development in the early years. There is solid evidence that, under the right conditions, better skills early in life make it easier to keep and acquire skills later on. For example, a child who received help with speech and language difficulties at Sure Start might have started Reception better able to communicate, as reflected in higher scores in communication and language at age 5. But that child would also find it easier to engage in class and make the most of the learning opportunities there. This could kick off a long-lasting ‘virtuous cycle’.
Complementing the direct effects on children, Sure Start services also sought to improve children’s home environments. A key focus of Sure Start was on providing additional support for parents, whether through stay-and-play sessions or more structured evidence-based parenting programmes. Some of our results suggest that Sure Start did affect children’s home environments. For example, a reduction in hospitalisations for accidents and injuries suggests that children were safer at home, while a reduction in unauthorised absences even in the early years suggests that parents may have made school attendance a higher priority.
Changing the relationship to services
Finally, Sure Start may have reshaped families’ relationship to services, ranging from accessing universal services such as healthcare to accessing specialist services for special educational needs or social care. Children who visited Sure Start centres were more ‘visible’ to service providers, meaning that there were more opportunities for early problems to be picked up and for families to be referred to – and supported to access – appropriate services. The impact this has on the outcomes that we measure is complex, and depends on whether early access to services increases service use in the long term (because families are more familiar with, and more known to, the system) or whether it decreases service use later in life (because early intervention prevents or reduces later issues). Our results on preventable hospitalisations, for example, suggest that families were more likely to access hospital services early in their child’s life, but that hospitalisations fell later on.
Sure Start reduced inequalities – in some outcomes
Sure Start services were designed to be available to all families in their local area, though the centres themselves were rolled out earlier and more intensively in disadvantaged areas.
There is a large evidence base suggesting that early years programmes are more effective for children from disadvantaged backgrounds. We find some evidence of this for Sure Start: impacts on hospitalisations, for example, are concentrated among children living in the poorest 30% of neighbourhoods. But in other cases, such as test scores, we find much smaller differences in Sure Start’s impacts between children who are and are not eligible for free school meals.
Sure Start’s impacts were often stronger for boys than for girls, particularly during adolescence. Virtually all of the decline in hospitalisations among teenagers was driven by Sure Start’s impacts on boys. Similarly, Sure Start’s benefits for GCSE results were almost twice as large for boys as they were for girls. We also find evidence that Sure Start had stronger effects on children from non-White backgrounds.
A cost-effective intervention
At its peak, Sure Start cost around £2.7 billion (in 2023–24 prices) per year. We find that the value to the public purse of the benefits that Sure Start created is around £2.4 billion – meaning that Sure Start directly defrayed a large portion of its cost, but did not (quite) ‘pay for itself’. However, the government was not the only beneficiary of Sure Start; the children and families using the centres also benefited directly, in the form of lower costs and higher lifetime earnings. These wider social benefits were worth around £3.1 billion per cohort, or around 11 times the long-run net cost of the programme (subtracting long-run savings to government from the up-front costs of the programme).
12.2 Lessons for policy
The main lesson that this evaluation holds for policymakers is that integrated early years services can have substantial, wide-ranging, long-lasting and financially valuable benefits for children’s lives. Bringing together a range of services in the early years was successful in reshaping children’s health, education, and social and emotional development. This is a prize worth having.
Our results also suggest that this was achieved precisely by bringing together and joining up services across a range of different areas. There is no one obvious candidate for a ‘magic bullet’ service; instead, Sure Start worked because it took seriously the academic evidence on the relationships between all the different dimensions of children’s development.
But this does not mean that any combination of services would be equally effective. Frustratingly, this evaluation can only shed indirect light on the role that different services played. While Sure Start staff on the ground put considerable effort into collecting data on who attended centres and which services they used, these data were often not valued by local or national government. In many cases, the data were not systematically collated even at the local authority level. In the places where data were collected, they have mostly been permanently deleted. This represents a real loss to evaluation and means that our understanding of how Sure Start worked is poorer than it could have been.
Our results do still suggest that Sure Start was effective for a wide range of children – but effects were somewhat stronger for those in disadvantaged neighbourhoods, for boys, and for children from ethnic minority backgrounds. This suggests that there may be some opportunity to prioritise services to some areas or types of children. At the same time, Sure Start generated significant financial benefits – for families and for the government – even in its universal, area-based model. There may well be benefits – to service take-up, to detection and prevention, to service quality, and to wider social capital – from continuing to use integrated early years services as a universal-within-area service that brings in families from many different backgrounds.
Looking forward
Since 2021, successive governments have signalled their interest in and commitment to integrated early years services through the Start for Life programme (focusing on conception to age 2) and a new network of Family Hubs (which serve children and young people up to age 19, and their families). Family Hubs have many similarities to Sure Start centres: they draw together services in education, public health, and parental work and benefits advice; they are an area-based service available to all families in their catchment area; and they maintain a key role for local authorities.
On the other hand, Family Hubs target a much wider age range than Sure Start centres did. This could offer benefits from continuing support even at older ages. But it also risks diluting the offer of support, especially since Family Hubs are much more lightly funded than Sure Start was. Family Hubs also place much more priority on virtual services and signposting rather than on in-person community hubs.
This evaluation of Sure Start suggests that integrated early years services can be an effective – and cost-effective – way to genuinely improve children’s outcomes in a range of areas, with long-lasting benefits. For a government that is committed to boosting school readiness, Sure Start provides encouraging evidence that a focus on family services could be a good place to start.
Appendix
Download a PDF of Appendix A.1-A.4 here.
References
Anderberg, D. and Olympiou, C., 2023. Children’s social care and early intervention policy: evidence from Sure Start. Economica, 90, 953–77.
Anders, J., Barr, A. C. and Smith, A. A., 2023. The effect of early childhood education on adult criminality: evidence from the 1960s through 1990s. American Economic Journal: Economic Policy, 15(1), 37–69.
Baker, M., Gruber, J. and Milligan, K, 2008. Universal child care, maternal labour supply and family well-being. Journal of Political Economy, 116(4), 709–45.
Belfield, C., Farquharson, C. and Sibieta, L., 2018. 2018 annual report on education spending in England. IFS Report, https://ifs.org.uk/publications/2018-annual-report-education-spending-england.
Blunt, I., 2013. Focus on preventable admissions: trends in emergency admissions for ambulatory care sensitive conditions, 2001 to 2013. QualityWatch.
Bolt, U., French, E., Hentall-MacCuish, J. and O’Dea, C., 2021. The intergenerational elasticity of earnings: exploring the mechanisms. IFS Working Paper W21/07, https://ifs.org.uk/publications/intergenerational-elasticity-earnings-exploring-mechanisms.
Bouchal, P. and Norris, E., 2014. Implementing Sure Start Children’s Centres. Institute for Government, https://www.instituteforgovernment.org.uk/sites/default/files/publications/Implementing%20Sure%20Start%20Childrens%20Centres%20-%20final_0.pdf.
Brewer, M., Cattan, S., Crawford, C. and Rabe, B., 2022. Does more free childcare help parents work more? Labour Economics, 74, 102100.
Britton, J., Farquharson, C. and Sibieta, L., 2019. 2019 annual report on education spending in England. IFS Report, https://ifs.org.uk/publications/2019-annual-report-education-spending-england.
Callaway, B. and Sant’anna, P. H. C., 2021. Difference-in-differences with multiple time periods. Journal of Econometrics, 225(2), 200–30.
Carneiro, P., Cattan, S., Conti, G., Crawford, C., Drayton, E., Farquharson, C. and Ridpath, N., 2024. The effect of Sure Start on youth misbehaviour, crime and contacts with children’s social care. IFS Report, https://ifs.org.uk/publications/effect-sure-start-youth-misbehaviour-crime-and-contacts-childrens-social-care.
Carneiro, P., Cattan, S. and Ridpath, N, 2024. The short- and medium-term impacts of Sure Start on educational outcomes. IFS Report, https://ifs.org.uk/publications/short-and-medium-term-impacts-sure-start-educational-outcomes.
Carneiro, P. and Ginja, R., 2014. Long-term impacts of compensatory preschool on health and behavior: evidence from Head Start. American Economic Journal: Economic Policy, 6, 135–73.
Carrell, S. and Hoekstra, M., 2010. Externalities in the classroom: how children exposed to domestic violence affect everyone’s kids. American Economic Journal: Applied Economics, 2(1), 211–28.
Cattan, S., Conti, G., Farquharson, C., Ginja, R. and Pecher, M., 2021. The health impacts of Sure Start. IFS Report, https://ifs.org.uk/publications/health-impacts-sure-start.
Cattan, S., Conti, G., Farquharson, C., Ginja, R. and Pecher, M., 2025. The health effects of universal early childhood interventions: evidence from Sure Start. IFS Working Paper 25/20, https://ifs.org.uk/publications/health-effects-universal-early-childhood-interventions-evidence-sure-start-0.
Children, Schools and Families Committee, 2010. Sure Start Children’s Centres. Fifth Report of Session 2009–10, House of Commons, https://publications.parliament.uk/pa/cm200910/cmselect/cmchilsch/130/13002.htm.
Conti, G., Heckman, J. J. and Pinto, R., 2016. The effects of two influential early childhood interventions on health and healthy behaviour. Economic Journal, 126, F28–65.
Cunha, F., Heckman, J. and Schennach, S. M., 2010. Estimating the technology of cognitive and noncognitive skill formation. Econometrica, 78(3), 883–931.
Currie, J., 2009. Healthy, wealthy, and wise: socioeconomic status, poor health in childhood, and human capital development. Journal of Economic Literature, 47, 87–122.
Daysal, N. M., Ding, H., Rossin-Slater, M. and Schwandt, H., 2024. Germs in the family: the short- and long-term consequences of intra-household disease spread. NBER Working Paper 29524.
Department for Education, 2025. Pupil absence in schools in England: 2023/24. https://explore-education-statistics.service.gov.uk/find-statistics/pupil-absence-in-schools-in-england/2023-24.
Department for Education and Employment, 1999. Sure Start: a guide for trailblazers.
Fort, M., Ichino, A. and Zanella, G., 2016. Cognitive and non-cognitive costs of daycare 0–2 for girls. Institute for the Study of Labor (IZA), Discussion Paper 9756, https://docs.iza.org/dp9756.pdf.
Fright, M. and Davies, N., 2023. Performance Tracker 2023: children’s social care. Institute for Government, https://www.instituteforgovernment.org.uk/publication/performance-tracker-2023/childrens-social-care.
Gaviria, A. and Raphael, S., 2001. School-based peer effects and juvenile behavior. Review of Economics and Statistics, 83(2), 257–68.
Goff, J., Hall, J., Sylva, K., Smith, T., Smith, G., Eisenstadt, N., Sammons, P., Evangelou, M., Smees, R. and Chu, K., 2013. Evaluation of Children’s Centres in England (ECCE): Strand 3: delivery of family services by Children’s Centres. Department for Education, Research Report DFE-RR297, https://assets.publishing.service.gov.uk/media/5a7cc90fe5274a2f304f00f4/DFE-RR297.pdf.
Hendren, N. and Sprung-Keyser, B., 2020. A unified welfare analysis of government policies. Quarterly Journal of Economics, 15, 1209–318.
HM Treasury, 1998. Comprehensive Spending Review 1998.
Hoare, P. and Beattie, T., 2003. Children with attention deficit hyperactivity disorder and attendance at hospital. European Journal of Emergency Medicine, 10(2), 98–100.
Hodge, L., Little, A. and Weldon, M., 2021. GCSE attainment and lifetime earnings. Department for Education, Research Report DFE-RR1131, https://assets.publishing.service.gov.uk/media/60c36f0cd3bf7f4bd11a2326/GCSE_Attainment_and_Lifetime_Earnings_PDF3A.pdf.
Maisey, R., Speight, S. and Haywood, S. with Hall, J., Sammons, P., Hussey, D., Goff, J., Evangelou, M. and Sylva, K., 2013. Evaluation of Children’s Centres in England (ECCE): Strand 2: baseline survey of families using Children’s Centres in the most disadvantaged areas. Department for Education, Research Report DFE-RR260, https://assets.publishing.service.gov.uk/media/5a7a3a8140f0b66a2fc00d2e/DFE-RR260.pdf.
Meadows, P. et al., 2011. National evaluation of Sure Start Local Programmes: an economic perspective. Department for Education, Research Report DFE-RR073, https://assets.publishing.service.gov.uk/media/5a7b2907ed915d429748d3d5/DFE-RR073.pdf.
Melhuish, E., Belsky, J., Leyland, A. H. and Barnes, J., 2008. Effects of fully-established Sure Start Local Programmes on 3-year-old children and their families living in England: a quasi-experimental observational study. The Lancet, 372, 1641–7.
National Audit Office, 2006. Sure Start Children’s Centres. HC 104 Session 2006–07, https://www.nao.org.uk/wp-content/uploads/2006/12/0607104.pdf.
National Audit Office, 2009. Sure Start Children’s Centres: memorandum for the Children, Schools and Families Committee. https://www.nao.org.uk/wp-content/uploads/2010/01/0910_sure_start_memorandum.pdf.
National Evaluation of Sure Start team, 2010. The impact of Sure Start Local Programmes on five year olds and their families. Department for Education, Research Report DFE-RR067, https://assets.publishing.service.gov.uk/media/5a7ae2d8e5274a319e77b6ac/DFE-RR067.pdf.
Pugh, G., 2010. The policy agenda for early childhood services. In G. Pugh and B. Duffy (eds), Contemporary Issues in the Early Years (5th edition), SAGE Publications Ltd.
Sammons, P., Hall, J., Smees, R. and Goff, J. with Sylva, K., Smith, T., Evangelou, M., Eisenstadt, N. and Smith, G., 2015. The impact of Children’s Centres: studying the effects of Children’s Centres in promoting better outcomes for young children and their families. Department for Education, Research Report DFE-RR495, https://assets.publishing.service.gov.uk/media/5a80acdb40f0b62305b8c838/DFE-RR495_Evaluation_of_children_s_centres_in_England__the_impact_of_children_s_centres.pdf
Smith, G., Field, K., Smith, T., Noble, S., Smith, T. and Plunkett, E., 2014. Evaluation of Children’s Centres in England (ECCE): the extent to which centres ‘reach’ eligible families, their neighbourhood characteristics and levels of use. Department for Education, Research Report DFE-RR358, https://assets.publishing.service.gov.uk/media/5a7ee6a240f0b6230268c3fd/RR358_-_FINALrevisedReachReport07042014.pdf.
Stewart, K., 2013. Labour’s record on the under fives: policy, spending and outcomes 1997-2010. Social Policy in a Cold Climate, Working Paper 4, https://sticerd.lse.ac.uk/dps/case/spcc/wp04.pdf.
Tunstill, J., Meadows, P., Allnock, D., Akhurst, S. and Garbers, C., 2005. Implementing Sure Start Local Programmes: an integrated overview of the first four years. Sure Start National Evaluation Report 10.
van den Berg, G. J. and Siflinger, B. M., 2022. The effects of a daycare reform on health in childhood: evidence from Sweden. Journal of Health Economics, 81, 102577.
Data
Department for Education. (2019). National Pupil Database. [data series]. 2nd Release. UK Data Service. SN: 2000108, DOI: http://doi.org/10.5255/UKDA-Series-2000108
Acknowledgements
This report provides a detailed overview of the short- and medium-term effects of Sure Start across a wide range of outcomes. It follows on from Cattan, Conti, Farquharson, Ginja and Pecher (2021) on the effect of Sure Start on hospitalisations, Carneiro, Cattan and Ridpath (2024) on the effect of Sure Start on educational outcomes and Carneiro, Cattan, Conti, Crawford, Drayton, Farquharson and Ridpath (2024) on the effect of Sure Start on youth offending, behaviour in school and interactions with children’s social care. For several outcomes across the reports, the methodology has been updated, which means some results have changed compared with prior reports. This report is therefore intended to supersede the earlier reports. A full outline of the changes to the methodology and the results can be found in Section A.2 of the appendix.
The authors are grateful for funding from the Nuffield Foundation (grant EDO /FR-000000372). The Nuffield Foundation is an independent charitable trust with a mission to advance social well-being. It funds research that informs social policy, primarily in Education, Welfare and Justice. The Nuffield Foundation is the founder and co-founder of the Nuffield Council on Bioethics, the Ada Lovelace Institute and the Nuffield Family Justice Observatory. The Nuffield Foundation has funded this project, but the views expressed are those of the authors and not necessarily the Foundation. Bluesky: @nuffieldfoundation.org | LinkedIn: Nuffield Foundation | Website: nuffieldfoundation.org. Co-funding from the ESRC-funded Centre for the Microeconomic Analysis of Public Policy (ES/T014334/1) is gratefully acknowledged.
This work contains statistical data from the Office for National Statistics (ONS) which are Crown Copyright. The use of the ONS statistical data in this work does not imply the endorsement of the ONS in relation to the interpretation or analysis of the statistical data. This work uses research datasets which may not exactly reproduce National Statistics aggregates. Analysis was carried out in the Secure Research Service, part of the Office for National Statistics.
We thank NHS Digital for providing access to the Hospital Episode Statistics under data sharing agreement CON-305762-B8S7B. This paper has been screened to ensure no confidential information is revealed.
Endnotes
Authors

Pedro Carneiro
Pedro is a Professor of Economics at University College London and an economist in the IFS' Centre for Microdata Methods and Practice (cemmap).

Sarah Cattan
Sarah is a Research Fellow at the Institute for Fiscal Studies.

Gabriella Conti
Gabriella is a Research Fellow of the IFS and a Professor of Economics in the Department of Economics and in the Department of Social Science at UCL.

Claire Crawford
Claire is a Research Fellow at IFS, working on the determinants and consequences of participation in childcare and education for parents and children.

Christine Farquharson
Christine's research examines inequalities in children's education and health, especially in the early education and childcare sector.

Nick Ridpath
Nick joined the IFS in 2023 and works in the Education and Skills sector, focusing on the long-run impacts of education policy.
More from IFS
Understand this issue



Policy analysis


Academic research


